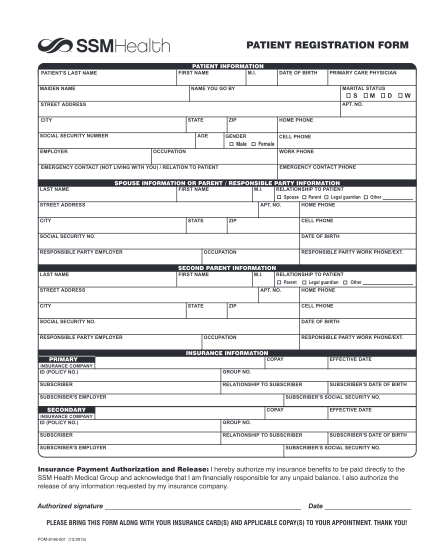
patient information update form
Patient registration patient information (first name) (street address) (city, state) (phone number) (e-mail address) (sex) (zip code) (cell phone number) (marital status) (date of birth) (middle initial) (last name) (please print) please present...
FILL NOW