demographic forms
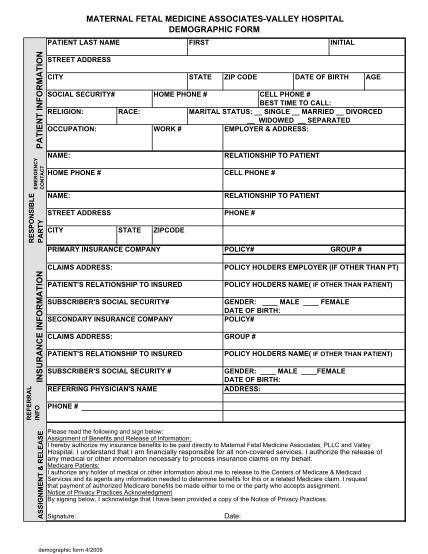
Maternal fetal medicine associates-valley hospital demographic form patient last name first initial patient information street address city social security# religion: occupation: race: work # state home phone # zip code date of birth age cell...
FILL NOW