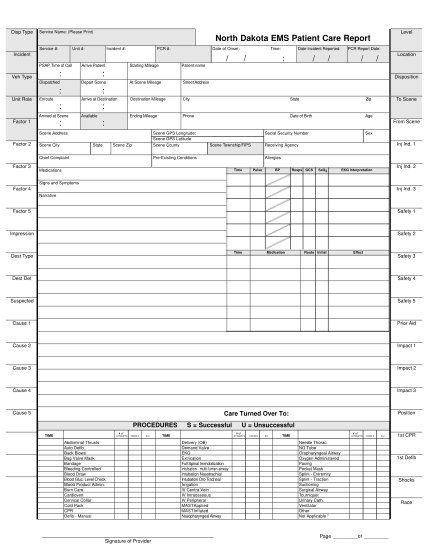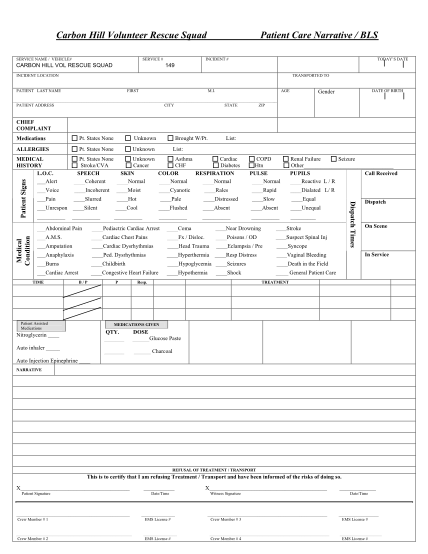
ems pcr template
Carbon hill volunteer rescue squad service name / vehicle# service # carbon hill vol rescue squad patient care narrative / bls incident # today?s date 149 incident location transported to patient last name first m.i. age date of birth gender...
FILL NOW