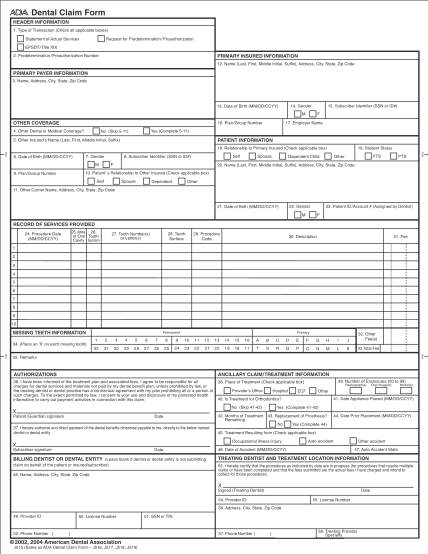
authorization to release x rays
X-ray request and release form date: / / patient name: requested by (if other then the patient): relationship to patient: exam date(s) requested: x-ray(s) to be sent/faxed to: i authorize the release of the x-rays(s) requested above. signature
FILL NOW