medical history cases pdf
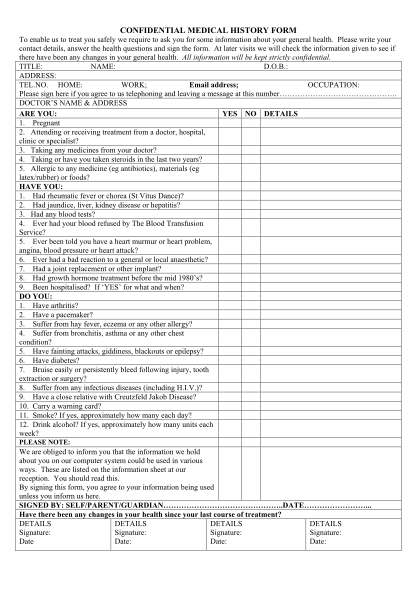
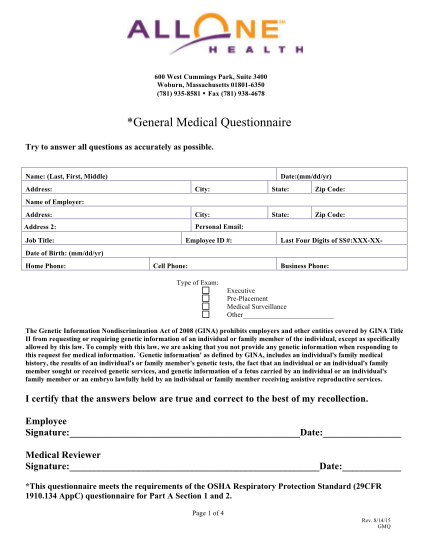
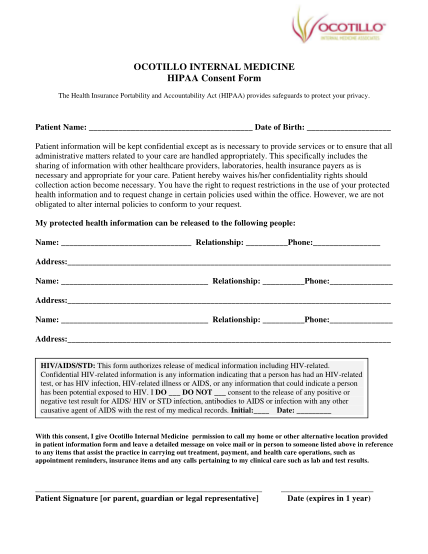
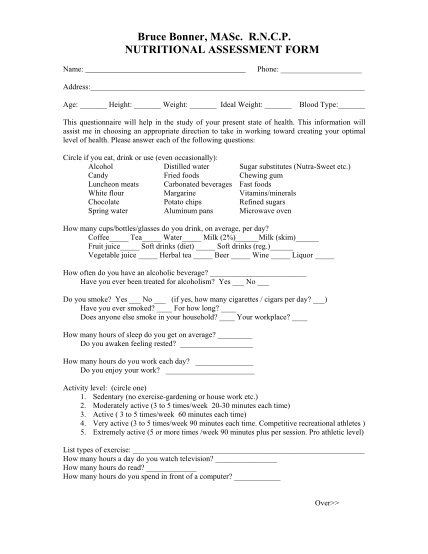
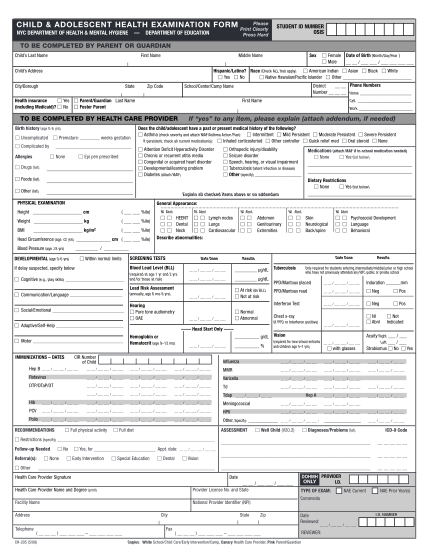
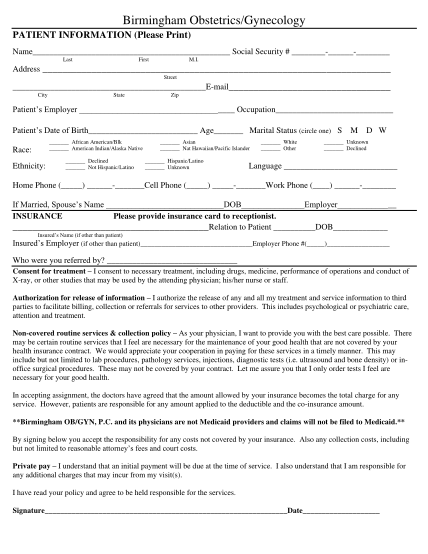
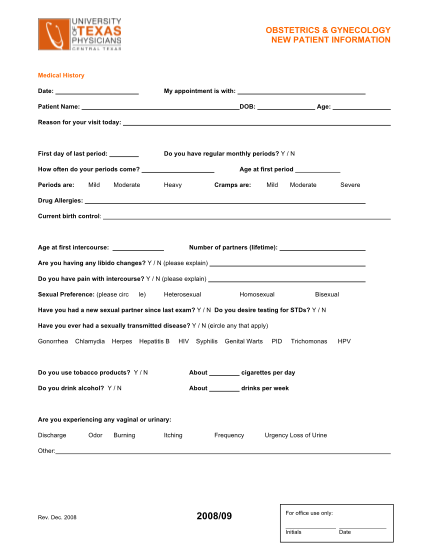
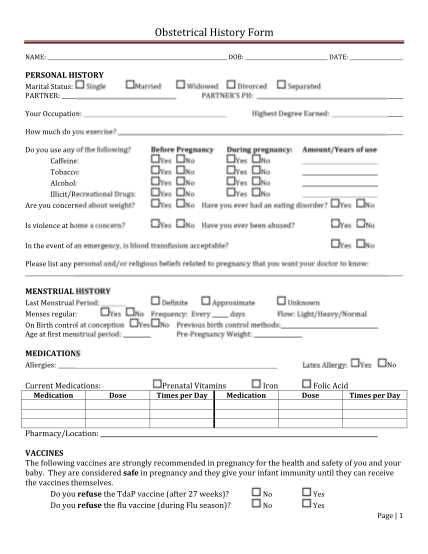
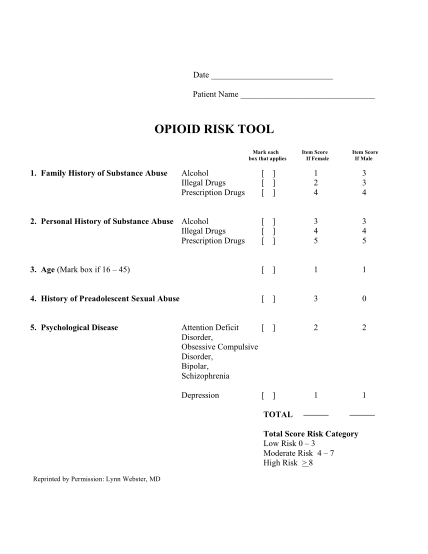
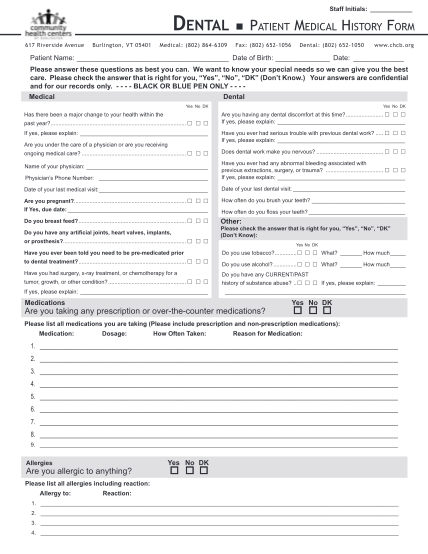
Patient medical history physician office phone date of last exam are you under a physicians care now? have you recently been hospitalized? are you taking any medications, pills, or drugs? do you take, or have you taken, phenfen or redux? have you...
FILL NOW