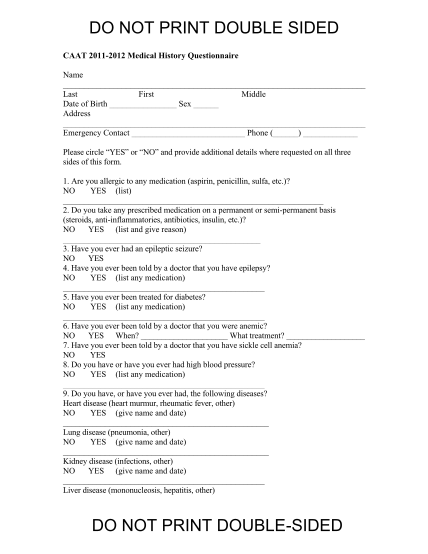
Sample Medical History Questionnaire
Jcc swimming medical history questionnaire name last first middle date of birth: sex: m or f please circle yes or no and provide additional details where requested on all three sides of this form. 1. are you allergic to any medication (aspirin, ,...
FILL NOW