Excel Dentistry Dental History Form - Excel Dentistry of Lewisville ...
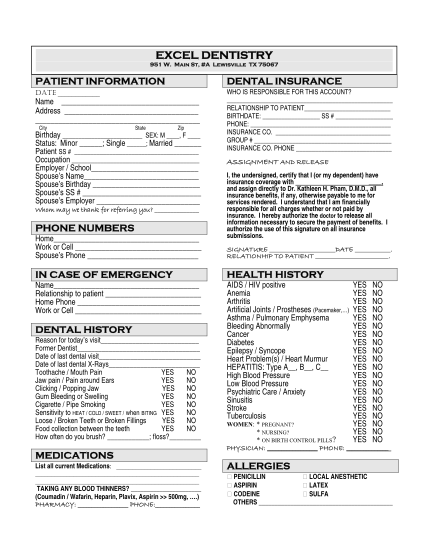
Excel dentistry 951 w. main st, #a lewisville tx 75067patient informationdental insurancedate who is responsible for this account? relationship to patient birthdate: ss # phone: insurance co. group # insurance co. phone name address...
FILL NOW