Membership Form - Family History Society of Buchan
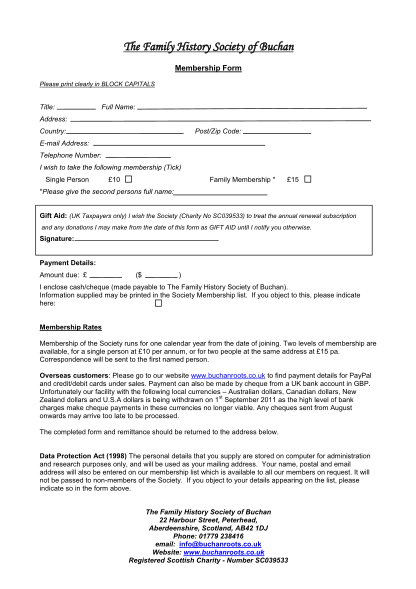
The family history society of buchan membership form please print clearly in block capitals title: full name: address: country: post/zip code: e-mail address: telephone number: i wish to take the following membership (tick) single person 10 family...
FILL NOW