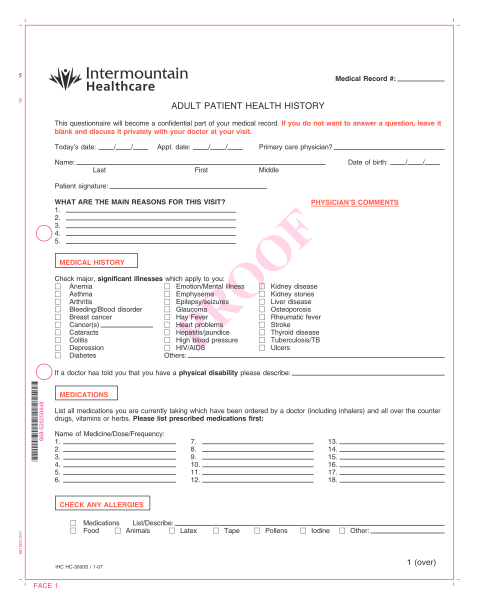
ADULT MEDICAL HISTORY FORM Name - Texas Family Physicians
6618 sitio del rio b-101 austin, texas 78730 phone: 512.524.2336 fax: 512.372.8525 adult medical history form name: sex: m f last first date of birth: age: middle i. past medical history yes no heart disease kidney disease asthma & lung liver,...
FILL NOW