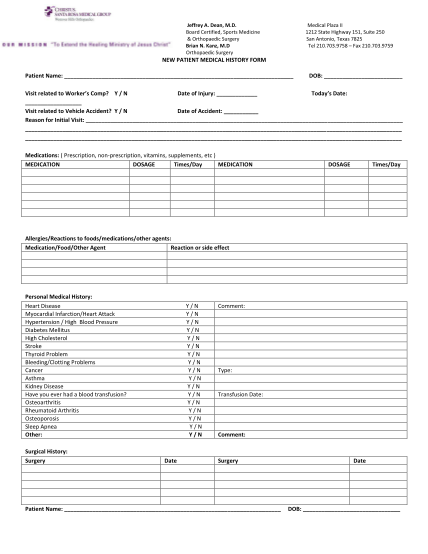
Adult medical history form - CC Orthodontics
Patient information form date: personal information patients title: mr. mrs. ms. dr. first name: preferred name: mi: last name: age: birth date: home address: occupation: gender: f m phone #: employer: business address: email: best daytime phone...
FILL NOW