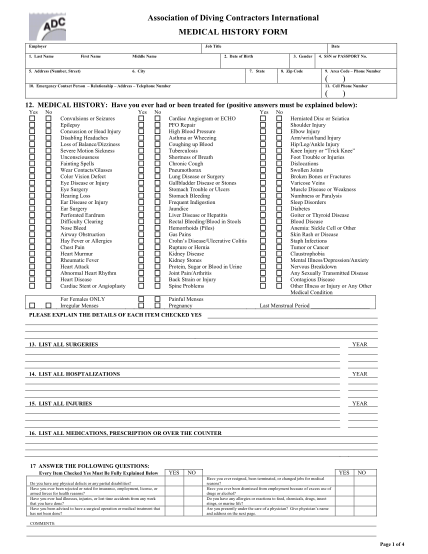
ADCI's REQUIRED medical history form
Association of diving contractors international medical history form employer job title 1. last name first name 5. address (number, street) middle name date 2. date of birth 6. city 3. gender 7. state 8. zip code 4. ssn or passport no. 9. area...
FILL NOW