Submitting an Out-of-Network Claim - VSP Vision Care
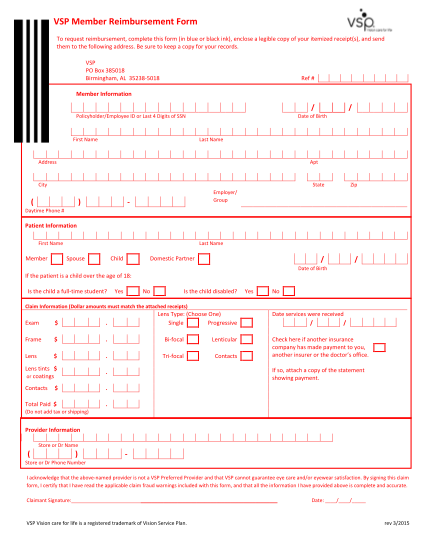
Out-of-network reimbursement form member information member's name date of birth address city state zip member's id or ssn name of group/employer patient information patient's name date of birth relationship to member if the patient is a child...
FILL NOW