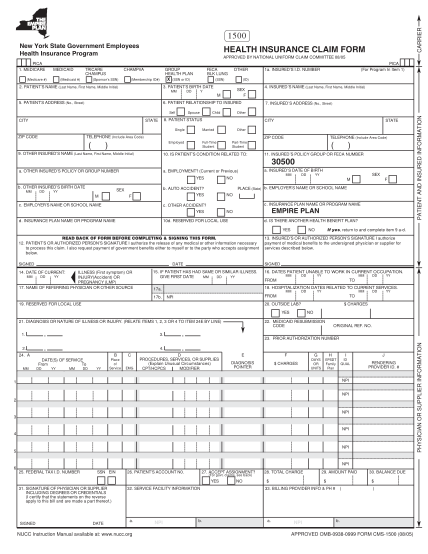
1500 claim
Revised cms-1500 health insurance claim form (08/05) comments added by the chirocode institute, .chirocode.com source of changes: .nucc.org/images/stories/pdf/final 1500 change log.pdf carrier physician or supplier information patient and insured...
FILL NOW