chiropractic superbill template
Original claim reference number. medical assistance health insurance. claim form. title xix program. a v. patient and
FILL NOW Original claim reference number. medical assistance health insurance. claim form. title xix program. a v. patient and
FILL NOW
Networknews november 2009 for health care professionals participating in the cigna and former great-west healthcare network h1n1 vaccine cigna to provide coverage to help reduce barriers for participants to receive the h1n1 vaccine, cigna is...
FILL NOW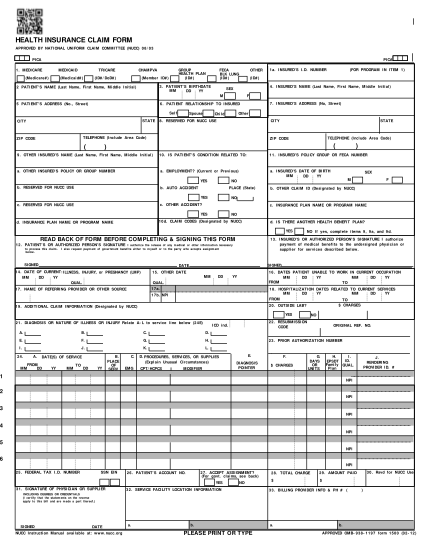
Nucc instruction manual available at: .nucc.org c. notice: any person who knowingly files a statement of claim containing any .. see http://.nubc. org/ for more information on ub-04 data element and printing
FILL NOW
The updated 1500 claim form: understanding its changes and the work to implement it tuesday, september 17, 2013 speakers ? kelly butler, emdeon, moderator ? nancy spector, ama ? claudette sikora, cms ? gloria davis, nextgen healthcare 2 objectives...
FILL NOW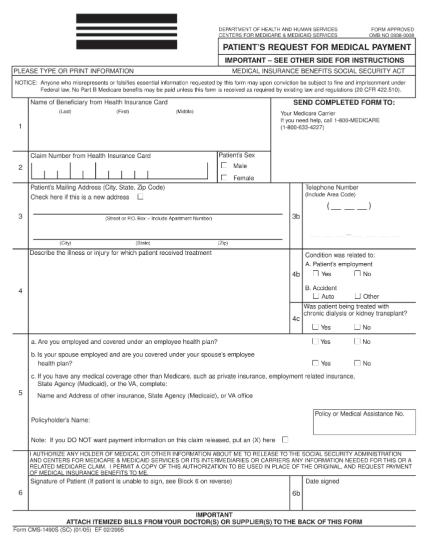
Department of health and human services centers for medicare & medicaid services form approved omb no 0938-8 patient's request for medical payment important see other side for instructions please type or print information medical insurance...
FILL NOW
Form cms 1500 at a glance the form cms-1500 is the standard paper claim form used by health care professionals and suppliers to bill medicare carriers or part a/b and durable medical equipment medicare administrative contractors (a/b macs and dme...
FILL NOW
Health insurance claim form. note: claims must be submittedwithin 3 months of being incurred to be eligible forreimbursement. 1. insured's name (last name, first name, middle initial). 8.patient's name (last name, first name, middle initial). 9....
FILL NOW Health insurance claim form. note: claims must be submittedwithin 3 months of being incurred to be eligible forreimbursement. 1. insured's name (last name, first name, middle initial). 8.patient's name (last name, first name, middle initial). 9....
FILL NOW Health insurance claim form. note: claims must be submittedwithin 3 months of being incurred to be eligible forreimbursement. 1. insured's name (last name, first name, middle initial). 8.patient's name (last name, first name, middle initial). 9....
FILL NOW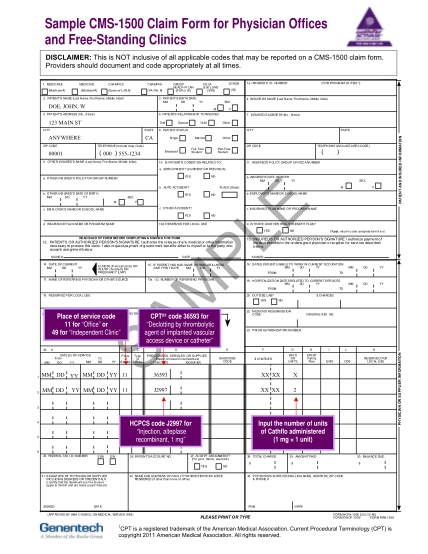
Sample cms-1500 claim form for physician offices and free-standing clinicsdisclaimer: this is not inclusive of all applicable codes that may be reported on a cms-1500 claim form. providers should document and code appropriately at all times.1....
FILL NOW Sample cms-1500 claim form for physician offices and free-standing clinicsdisclaimer: this is not inclusive of all applicable codes that may be reported on a cms-1500 claim form. providers should document and code appropriately at all times.1....
FILL NOW Sample cms-1500 claim form for physician offices and free-standing clinicsdisclaimer: this is not inclusive of all applicable codes that may be reported on a cms-1500 claim form. providers should document and code appropriately at all times.1....
FILL NOW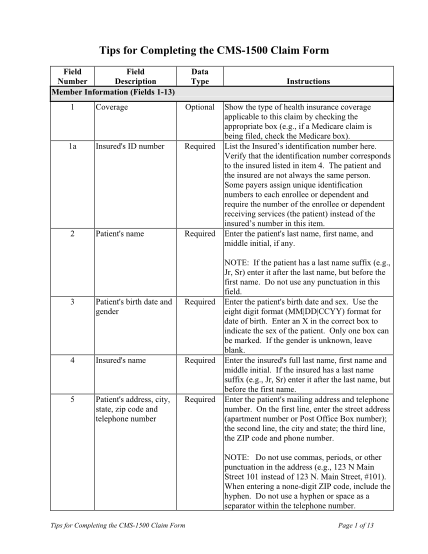
Tips for completing the cms-1500 claim formfield field number description member information (fields 1-13) 1 coverage data type optional instructions show the type of health insurance coverage applicable to this claim by checking the appropriate...
FILL NOW Tips for completing the cms-1500 claim formfield field number description member information (fields 1-13) 1 coverage data type optional instructions show the type of health insurance coverage applicable to this claim by checking the appropriate...
FILL NOW
May 2, 2011 information or white out. note: the following examples are in black and white. an original cms-1500 claim form is printed in red. drop out ink
FILL NOW