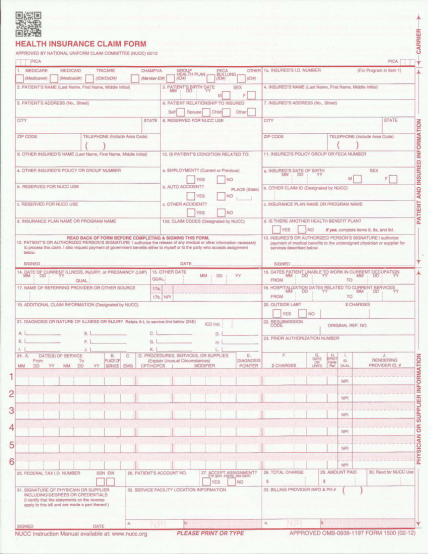
officemate 1500 forms
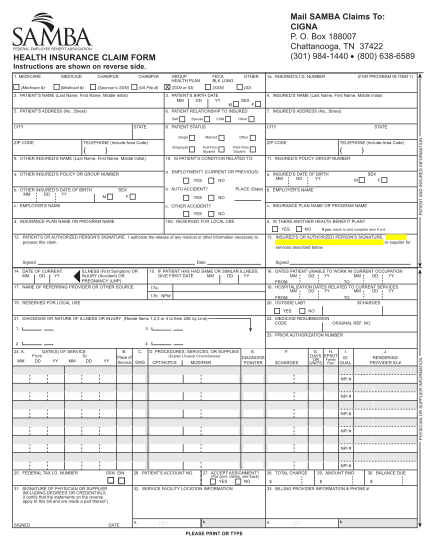
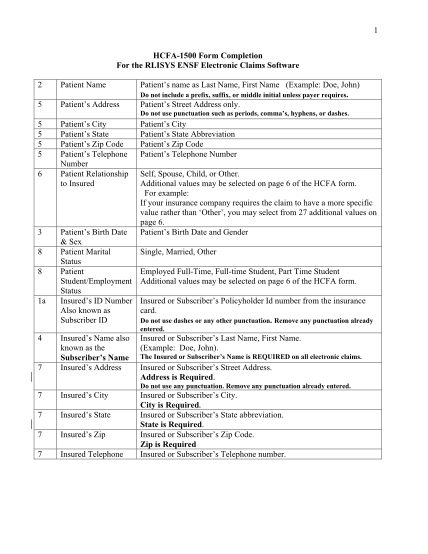
1 hcfa-1500 form completion for the rlisys ensf electronic claims software 2 patient name patient s name as last name, first name (example: doe, john) do not include a prefix, suffix, or middle initial unless payer requires. 5 patient s address...
FILL NOW