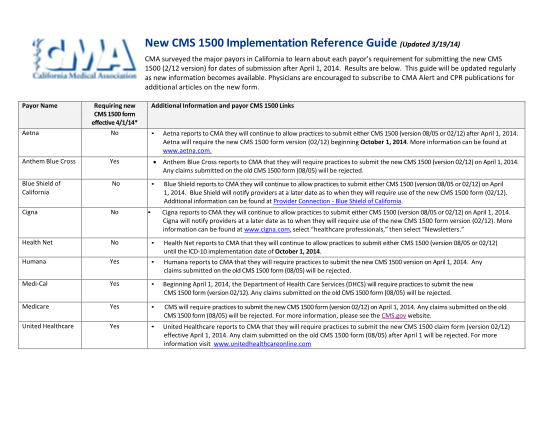
CMS 1500 FORM FOR CALIFORNIA WORKERS COMPENSATION. CMS 1500 FORM FOR CALIFORNIA WORKERS COMPENSATION - slidemanuals
Cms 1500 form for california workers compensation slidemanuals.party download deciphering the new cms 1500 claim form pdf download cms 1500 staples inc pdf download cms 1500 form california victim compensation and pdf download medical forms...
FILL NOW