1000 great west dr kennett mo
Sign form - return to patient. forward completed claim forms to: 1 great- west drive. kennett, mo 63857-3749. vision claim form. part a - member
FILL NOW Sign form - return to patient. forward completed claim forms to: 1 great- west drive. kennett, mo 63857-3749. vision claim form. part a - member
FILL NOW
591692c medical claim form cigna download : 591692c medical claim form cigna 591692c medical claim form cigna use this form for all medical plans. you can find dental and pharmacy claim forms on mycigna. go to: review my coveragedental or...
FILL NOW
Cigna healthcare - medication prior authorization form pharmacy services notice: failure to complete this form in its entirety may result in delayed processing or an adverse determination for insufficient information. phone: (800)244-6224 fax:...
FILL NOW
Form information cigna vision claim form insured and/or administered by connecticut general life insurance company cigna healthcare important: this claim form is intended for subscribers and covered dependents who receive services from providers...
FILL NOW
Cigna vision claim form cigna healthcare important: this claim form is intended for subscribers and covered dependents who receive services from providers outside the cigna vision network. if your plan permits a non-participating provider to...
FILL NOW
Gw prescription drug claim form reason for reimbursement this claim form can be used to request reimbursement of covered expenses. please check which reason applies (at least one must be checked): eligibility (please explain) emergency...
FILL NOWMember claim form insured and/or administered by connecticut general life insurance company cigna health and life insurance company cigna behavioral health, inc. cigna healthcare* not to be used for pharmacy or dental claims this form can be used...
FILL NOW
35. remarks. j400 (same as ada dental claim form j401, j402, j403, j404). to reorder call 1-800-947-4746 or go online at .adacatalog.org. 1 2 3
FILL NOW
Dental claim form header information 1. type of transaction (check all applicable boxes) statement of actual services request for predetermination / preauthorization epsdt/ title xix primary insured information 2. predetermination /...
FILL NOW
Clear fields form information member claim form insured and/or administered by connecticut general life insurance company not to be used for pharmacy or dental claims cigna healthcare this form can be used for all medical plans. this form only...
FILL NOW Clear fields form information member claim form insured and/or administered by connecticut general life insurance company not to be used for pharmacy or dental claims cigna healthcare this form can be used for all medical plans. this form only...
FILL NOW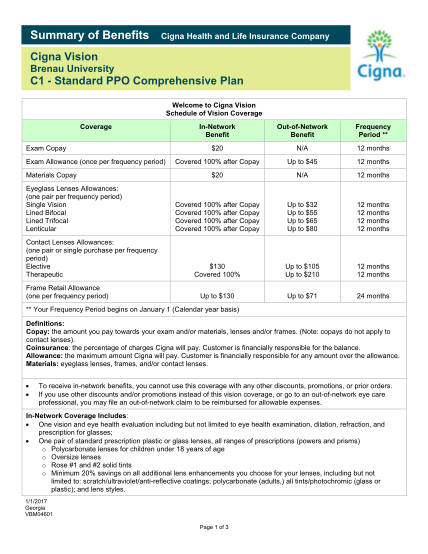
Summary of benefitscigna health and life insurance companycigna vision brenau universityc1 standard ppo comprehensive plan welcome to cigna vision schedule of vision coverage coverage exam copay exam allowance (once per frequency period) materials...
FILL NOW
Cigna vision claim formimportant: this claim form is intended for subscribers and covered dependents who receive services from providers outsidethe cigna vision network. if your plan permits a non-participating provider to accept assignment, the...
FILL NOW
Member claim form insured and/or administered by cigna behavioral health, inc. not to be used for medical, pharmacy or dental claims this form can be used for all behavioral plans. this form only needs to be completed if the provider is not...
FILL NOW
Group dental claim form insured and/or administered by connecticut general life insurance company cigna dental borgwarner inc. mail this form to: cigna healthcare service center p.o. box 188036 chattanooga, tn 37422-8036 telephone: 1--336-8258...
FILL NOW