866 873 8279
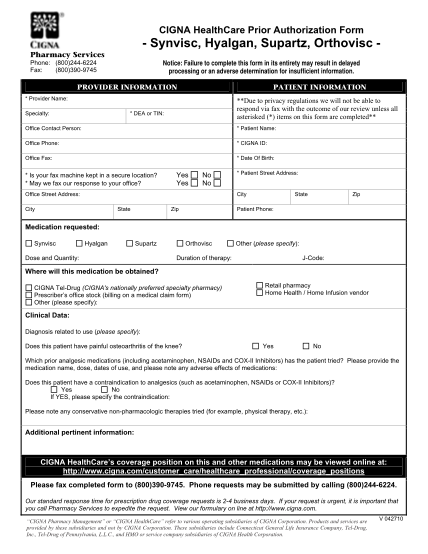
Cigna healthcare - medication prior authorization form pharmacy services notice: failure to complete this form in its entirety may result in delayed processing or an adverse determination for insufficient information. phone: (800)244-6224 fax:...
FILL NOW