Cigna Dental Claim Form - Creativa Associates
35. remarks. j400 (same as ada dental claim form j401, j402, j403, j404). to reorder call 1-800-947-4746 or go online at .adacatalog.org. 1 2 3
FILL NOW 35. remarks. j400 (same as ada dental claim form j401, j402, j403, j404). to reorder call 1-800-947-4746 or go online at .adacatalog.org. 1 2 3
FILL NOW
Dental claim form header information 1. type of transaction (check all applicable boxes) statement of actual services request for predetermination / preauthorization epsdt/ title xix primary insured information 2. predetermination /...
FILL NOW
Clear fields form information member claim form insured and/or administered by connecticut general life insurance company not to be used for pharmacy or dental claims cigna healthcare this form can be used for all medical plans. this form only...
FILL NOW
Group dental claim form insured and/or administered by connecticut general life insurance company cigna dental borgwarner inc. mail this form to: cigna healthcare service center p.o. box 188036 chattanooga, tn 37422-8036 telephone: 1--336-8258...
FILL NOW
Insured and/or administered by connecticut general life insurance company group dental claim form cigna healthcare vermont state colleges, inc. mail this form to: cigna healthcare p.o. box 188036 chattanooga, tn 37422-8036 telephone: 1--336-8258...
FILL NOW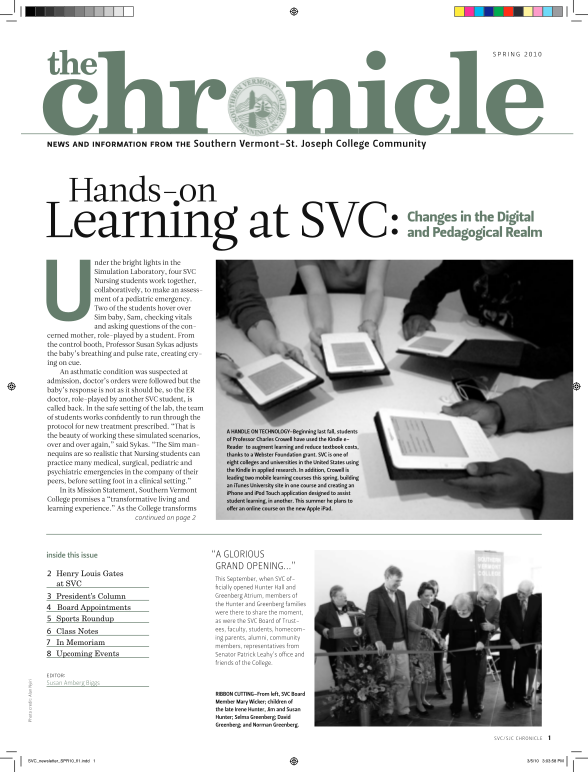
Form information dental claim form header information 1. type of transaction (mark all applicable boxes) statement of actual services request for predetermination / preauthorization for mailing address, call customer service at 1-800-244-6224...
FILL NOW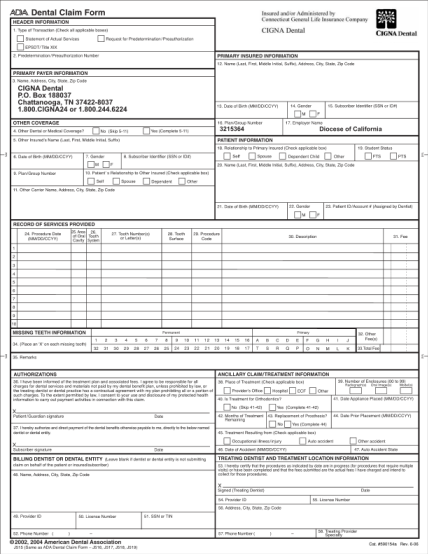
Dental claim form header information 1. type of transaction (check all applicable boxes) statement of actual services epsdt/ title xix 2. predetermination / preauthorization number request for predetermination / preauthorization primary insured...
FILL NOW
Out-of-network claims can be submitted by the provider if the provider is able and willing to file on your
FILL NOW
Cigna predetermination forms.pdf download here number 2006 american dental association http://.cigna.com/pdf/forms dental claim.pdf dental claim form 1. statement of actual services request for predetermination/preauthorization 2006 american and...
FILL NOW
Important: this claim form is intended for subscribers and covered completed cms-1500 form (also known as a hcfa-1500 form) to cigna vision at the
FILL NOW
Neuron direct billing claim form - optical section 1 - provider name and code (to be completed by provider 's personnel) provider name provider code section 2 - member 's details (to be completed by provider 's personnel) membership no. member 's...
FILL NOW
Sep 30, 2005 tive and business offices of the college cocoa is also the home of the 919. 559. 93. 821. 612. the accompanying notes are an integral part of this statement wide fmaneial statements see note below for description
FILL NOW
Claim formto be used for outofnetwork medical claimsand for all dental and vision claimsunder the cignalinksmiddle east programme.section a. important information: please readplease complete and sign this claim form, and submit it along with...
FILL NOW
Health insurance claim form instructions are shown on reverse side. 1. medicare (medicare #) medicaid (medicaid #) champus (sponsor's ssn) champva (va file #) mail samba claims to: cigna p. o. box 188007 chattanooga, tn 37422 (301) 984-1440 (800)...
FILL NOW
Uft welfare fund c/0. connecticut general. life insurance co. cigna healthcare. dental form. m t't':d rrderiaritin or t?al7he)ts. welfare fund
FILL NOW