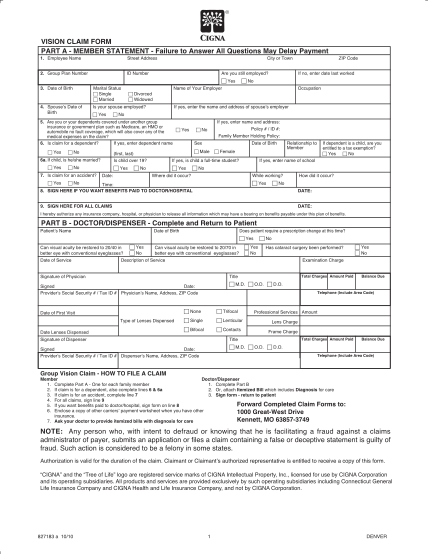
1000 great west dr kennett mo
Sign form - return to patient. forward completed claim forms to: 1 great- west drive. kennett, mo 63857-3749. vision claim form. part a - member
FILL NOW Sign form - return to patient. forward completed claim forms to: 1 great- west drive. kennett, mo 63857-3749. vision claim form. part a - member
FILL NOW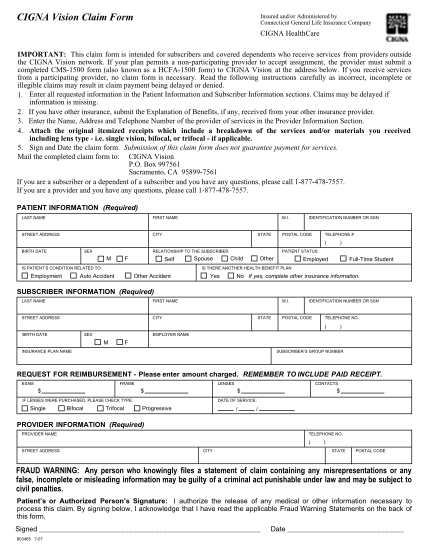
Form information cigna vision claim form insured and/or administered by connecticut general life insurance company cigna healthcare important: this claim form is intended for subscribers and covered dependents who receive services from providers...
FILL NOW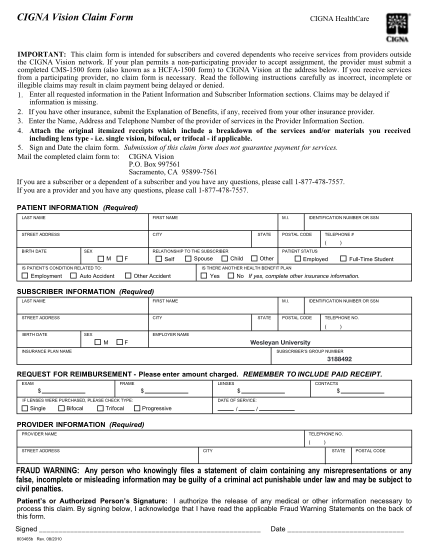
Cigna vision claim form cigna healthcare important: this claim form is intended for subscribers and covered dependents who receive services from providers outside the cigna vision network. if your plan permits a non-participating provider to...
FILL NOW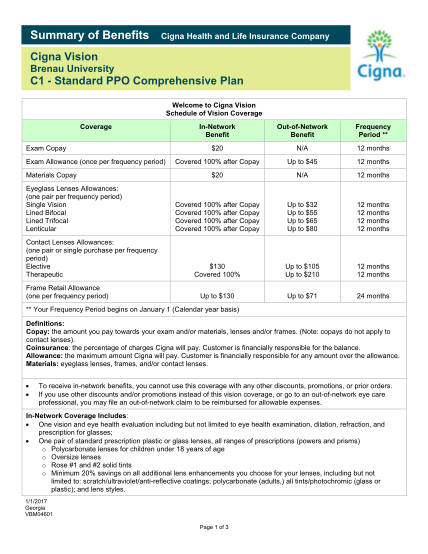
Summary of benefitscigna health and life insurance companycigna vision brenau universityc1 standard ppo comprehensive plan welcome to cigna vision schedule of vision coverage coverage exam copay exam allowance (once per frequency period) materials...
FILL NOW
Cigna vision claim formimportant: this claim form is intended for subscribers and covered dependents who receive services from providers outsidethe cigna vision network. if your plan permits a non-participating provider to accept assignment, the...
FILL NOW
Please return your completed claim form to: for claim forms outside the usa, cigna, international claims, 1 knowe road, greenock pa15 4rj tel: +44 (0) 1475 492197 fax: +44 (0) 1475 492424 email address: ice.team cigna.com for claim forms in the...
FILL NOW
Cigna global health options medical and vision claim form patients details to be completed by the beneficiary or his/her legal representative 1 patient name 2 policy id 3 patients date of birth 4 full mailing address of patient 5 state nature of...
FILL NOW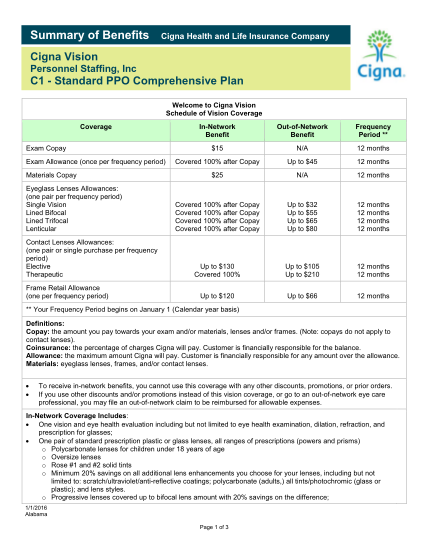
Summary of benefitscigna health and life insurance companycigna vision personnel staffing, incc1 standard ppo comprehensive plan welcome to cigna vision schedule of vision coverage coverage exam copay exam allowance (once per frequency period)...
FILL NOW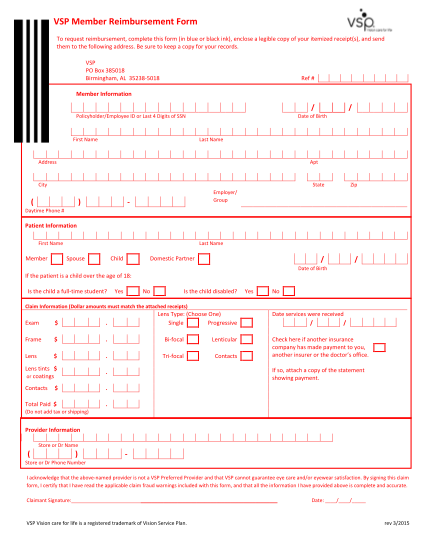
Out-of-network reimbursement form member information member's name date of birth address city state zip member's id or ssn name of group/employer patient information patient's name date of birth relationship to member if the patient is a child...
FILL NOW
Dental claim form header information 1. type of transaction (check all applicable boxes) statement of actual services epsdt/ title xix 2. predetermination / preauthorization number request for predetermination / preauthorization primary insured...
FILL NOW
Wells fargo insurance services independent business owners program office use only cigna vision enrollment form website independent business owners, spouses and families mail your completed enrollment form to wells fargo insurance services, p. o....
FILL NOW
Out-of-network claims can be submitted by the provider if the provider is able and willing to file on your
FILL NOW
Step 2: allergies & health conditions complete this section every time. cigna home delivery pharmacy. prescription order form. 1 2 3 4 a b c d.
FILL NOW
Important: this claim form is intended for subscribers and covered completed cms-1500 form (also known as a hcfa-1500 form) to cigna vision at the
FILL NOW
Cigna vision claim formcigna healthcareimportant: this claim form is intended for subscribers and covered dependents who receive services from providers outsidethe cigna vision network. if your plan permits a nonparticipating provider to accept...
FILL NOW