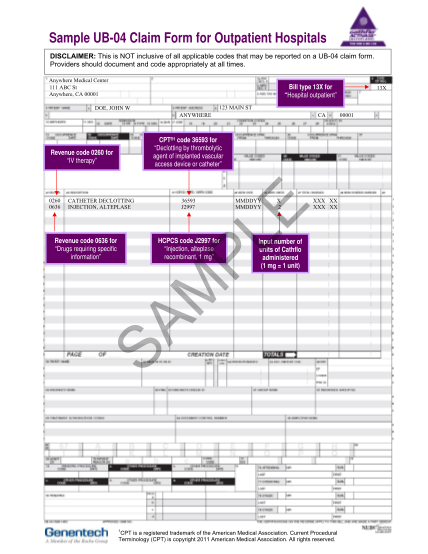
ub 04 to 837i mapping
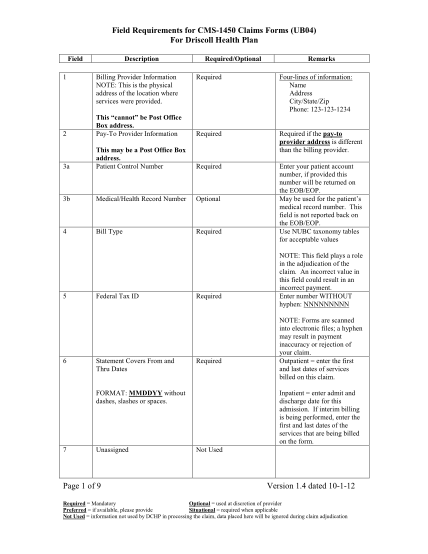
Trailblazer health enterprises education makes the difference cms-1450 claim form crosswalk to the ansi 837i version 5010a2 the implementation of the ansi 837i v5010a2 institutional health care claim presents substantial changes in the content of...
FILL NOW