dacum chart template
Dacum research chart for massage therapist. duties. tasks. a. perform. patient/client. assessment. a-1 take patient/client health history. a-2 review
FILL NOW Dacum research chart for massage therapist. duties. tasks. a. perform. patient/client. assessment. a-1 take patient/client health history. a-2 review
FILL NOW
Designed using perform pro, whs/dior, jun 94 adobe professional 7.0 dd form 314, dec 53 preventive maintenance 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 nomenclature model assigned to registration number...
FILL NOW
Maternal fetal medicine associates-valley hospital demographic form patient last name first initial patient information street address city social security# religion: occupation: race: work # state home phone # zip code date of birth age cell...
FILL NOW
Delta dental of californiastate government programsperiodontal evaluation chartp.o. box 537010sacramento, ca 958537010(800) 8384337patient namecharting datepatient date of birthprovider namepatient id numberlicense numbernational provider...
FILL NOW Delta dental of californiastate government programsperiodontal evaluation chartp.o. box 537010sacramento, ca 958537010(800) 8384337patient namecharting datepatient date of birthprovider namepatient id numberlicense numbernational provider...
FILL NOW
Dear patient, welcome to the dignity health medical group nevada henderson clinic. you are scheduled to see: o dr. emily peterson on (today s date) at (appointment time) am/pm co-payment policy your co-payment, if applicable, is due at the time of...
FILL NOW
New york state department of health division of assisted living assisted living residence medical evaluation all spaces must be filled out resident's name: date of exam: facility name: date of birth: sex: present home address: street city state...
FILL NOW
Name: date: doubleentry chart for watching a film directions: use the chart below as you watch to record and consider the aspects that you find most important or interesting. first, on the left side, note a specific quote or detail from the film;...
FILL NOW
Medication and allergy tracking chart. this chart can help you keep track of the medicines prescriptions, over-the-counter medicines, herbs, vitamins or
FILL NOW Medication and allergy tracking chart. this chart can help you keep track of the medicines prescriptions, over-the-counter medicines, herbs, vitamins or
FILL NOW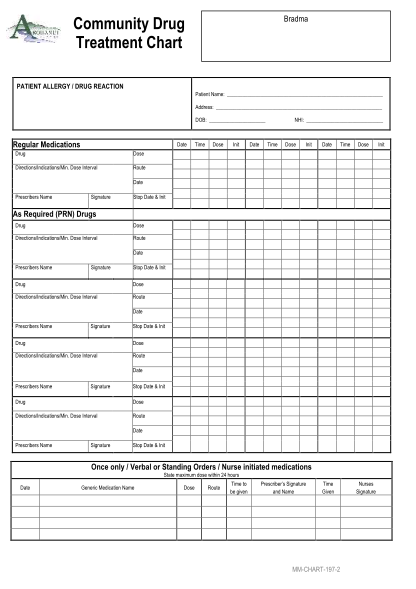
Bradma community drug treatment chart patient allergy / drug reaction patient name: address: dob: regular medications date drug dose init date time dose init date time dose dose directions/indications/min. dose interval time nhi: route date...
FILL NOW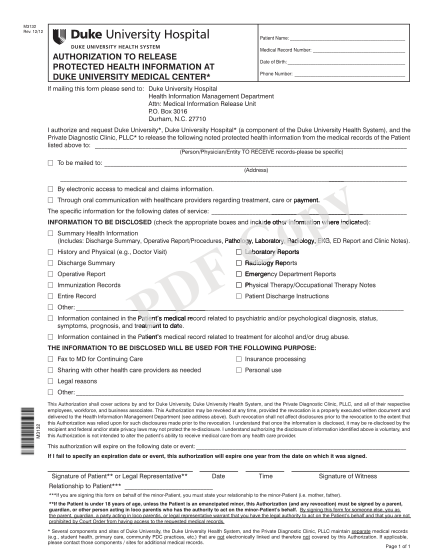
M3132 rev. 12/12 patient name: medical record number: authorization to release protected health information at duke university medical center* date of birth: phone number: if mailing this form please send to: duke university hospital
FILL NOW
Office site #nh one elliot way manchester, nh 03103 patient identification 1070 holt avenue, suite 1400 manchester, nh 03109 release of healthcare information name: date of birth: address: zip phone: authorization to: release patient information...
FILL NOW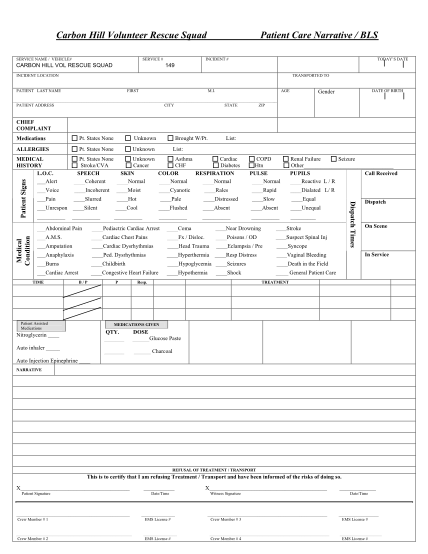
Carbon hill volunteer rescue squad service name / vehicle# service # carbon hill vol rescue squad patient care narrative / bls incident # today?s date 149 incident location transported to patient last name first m.i. age date of birth gender...
FILL NOW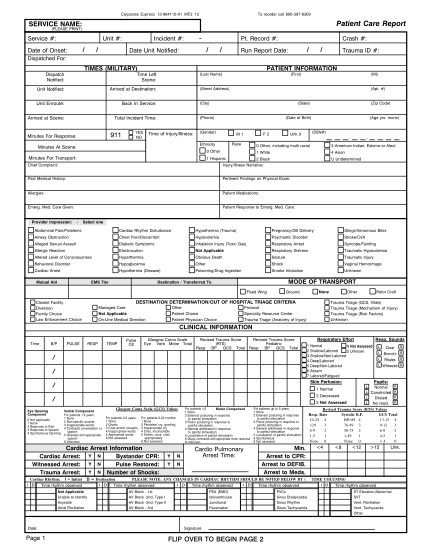
Patient care report. service name: (please print). service #: unit #: incident #: date of onset: date unit notified: pt. record #: crash #: run report date:
FILL NOW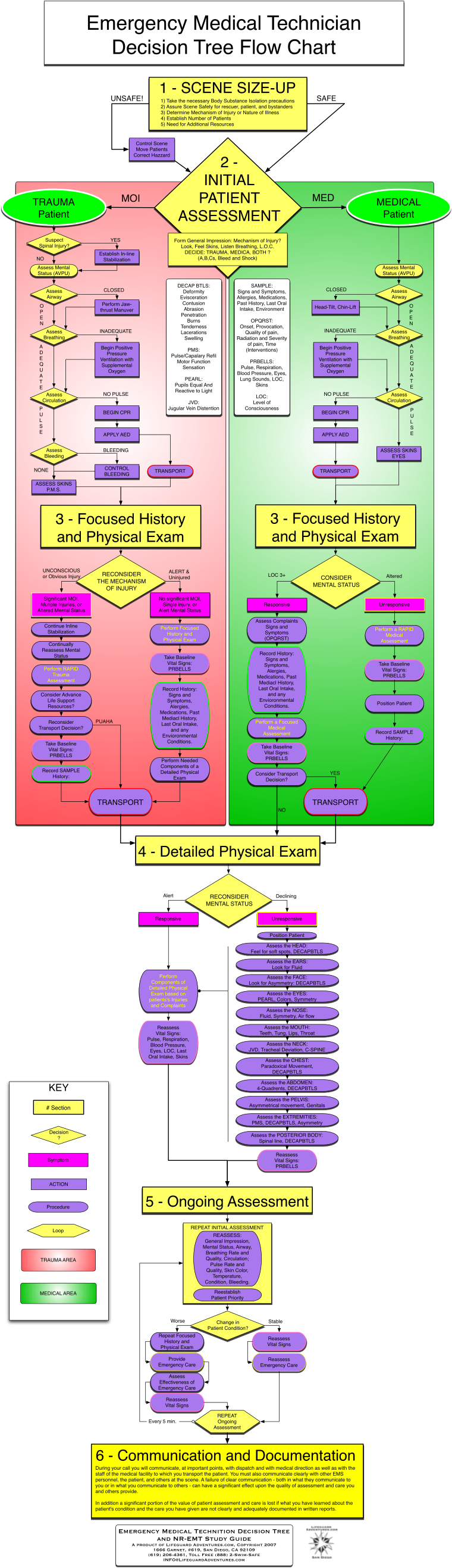
Mediacl history,. last oral intake, and any. envioronmental. conditions. perform focused. history and. physical exam. take baseline. vital signs: prbells
FILL NOW Mediacl history,. last oral intake, and any. envioronmental. conditions. perform focused. history and. physical exam. take baseline. vital signs: prbells
FILL NOW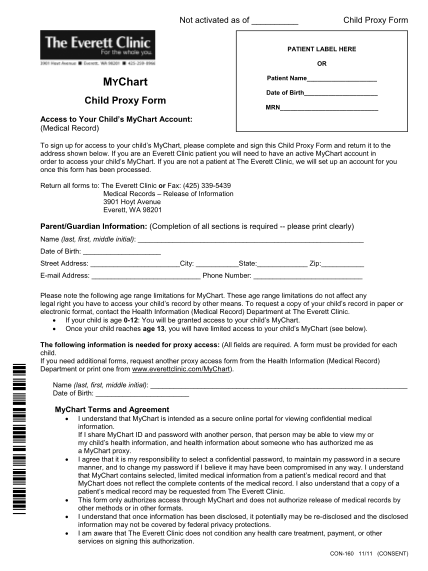
Not activated as of child proxy form patient label here or mychart child proxy form access to your child's mychart account: (medical record) patient name date of birth mrn to sign up for access to your child's mychart, please complete and sign...
FILL NOW
State of texas interagency eye examination report. examination report. patient's name: date of birth: address: city: state: zip code: parent/spouse name:
FILL NOW
Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW Staple 2-hole 1/4 2 3/4 c-to-c intensive outpatient program 3-hole 1/4 4 1/4 c-to-c admission face sheet patient label patient name: last: first: middle: are you known by any other name? no yes: mother's maiden name: patient
FILL NOW
Name: date: 1 chart: university of washington school of dentistry - medical and dental history general information male c. weight: lbs. month day year female d. height: ft. inches e. highest grade of regular school that you have completed? f....
FILL NOW Name: date: 1 chart: university of washington school of dentistry - medical and dental history general information male c. weight: lbs. month day year female d. height: ft. inches e. highest grade of regular school that you have completed? f....
FILL NOW Name: date: 1 chart: university of washington school of dentistry - medical and dental history general information male c. weight: lbs. month day year female d. height: ft. inches e. highest grade of regular school that you have completed? f....
FILL NOW Name: date: 1 chart: university of washington school of dentistry - medical and dental history general information male c. weight: lbs. month day year female d. height: ft. inches e. highest grade of regular school that you have completed? f....
FILL NOW Name: date: 1 chart: university of washington school of dentistry - medical and dental history general information male c. weight: lbs. month day year female d. height: ft. inches e. highest grade of regular school that you have completed? f....
FILL NOW