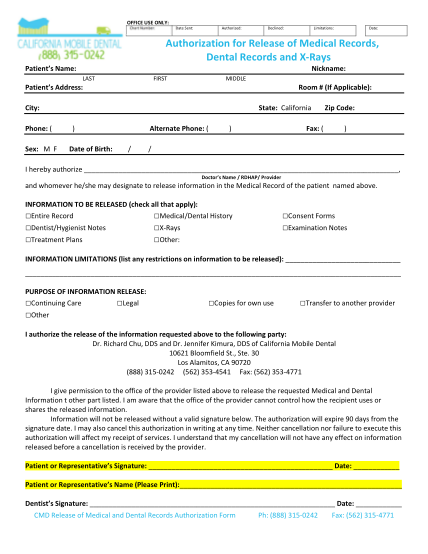
5) Record Release Authorization Form - California Mobile Dental
Office use only: chart number: date sent: authorized: declined: limitations: date: authorization for release of medical records, dental records and x-rays patient s name: nickname: last first middle patient s address: room # (if applicable): city:...
FILL NOW