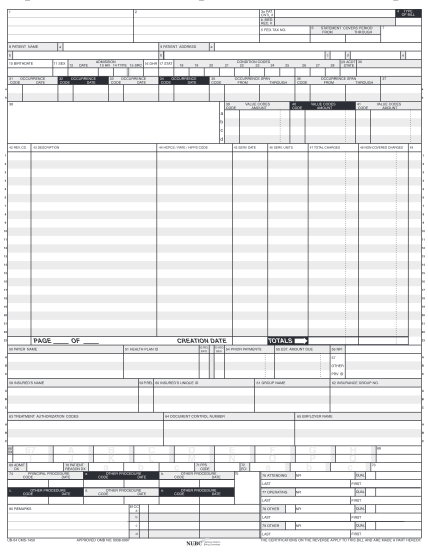
treatment administration record
Request for level ii pasrr evaluation and determination or resident review section i: request information date: request for: initial level ii evaluation and determination or resident review from: agency: phone: to: agency: phone: an indication of,...
FILL NOW