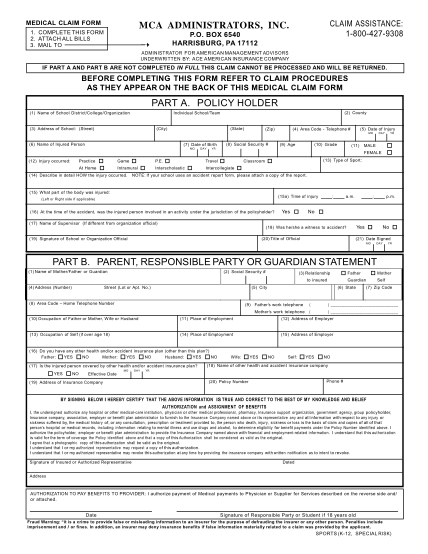
mca administrators claims address
Medical claim form claim assistance: 1-800-427-9308 mca administrators, inc. 1. complete this form 2. attach all bills 3. mail to p.o. box 6540 harrisburg, pa 17112 ? administrator for american management advisors underwritten by: ace american...
FILL NOW