CIGNA Medical Claim Form-Scranton
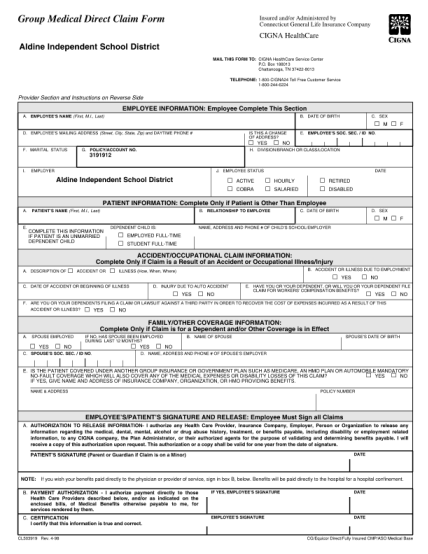
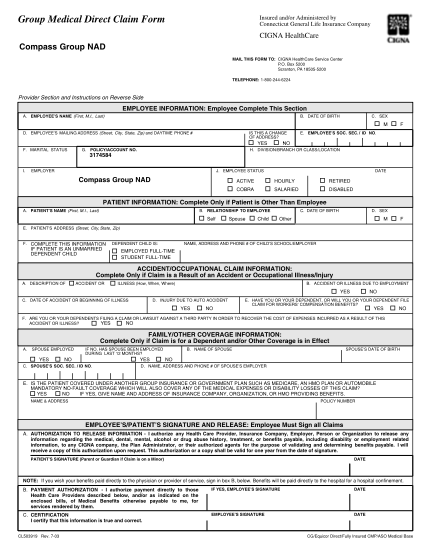
Group medical direct claim form insured and/or administered by connecticut general life insurance company cigna healthcare compass group nad mail this form to: cigna healthcare service center p.o. box 5200 scranton, pa 18505-5200 telephone:...
FILL NOW