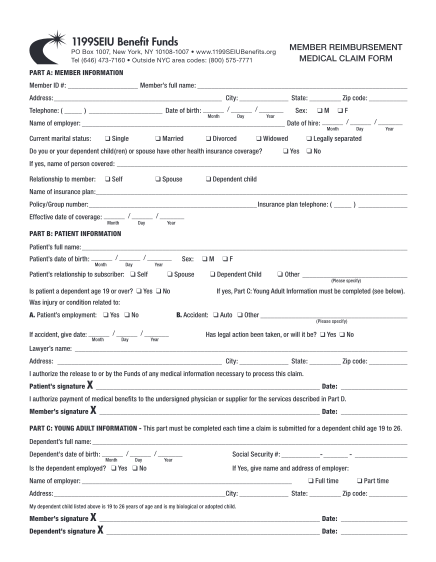
( ) MASTER MEDICAL CLAIM FORM - oakland
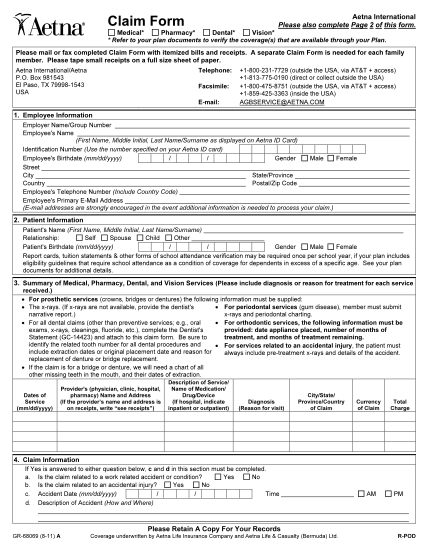
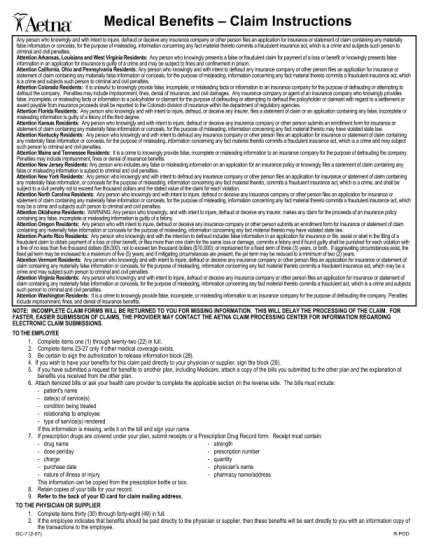
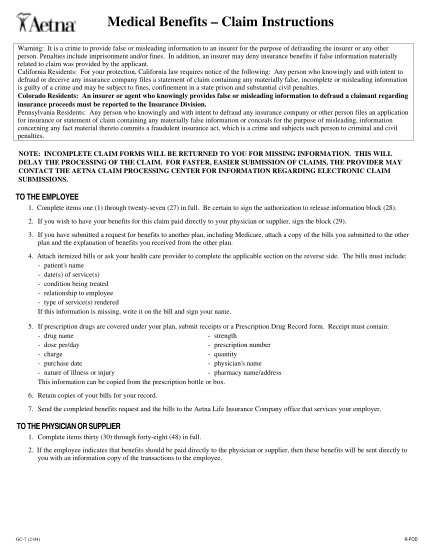
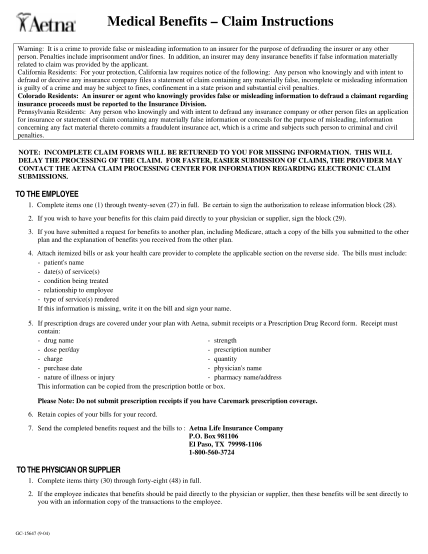
Master medical claim form an independent licensee of the blue cross and blue shield association. cl instructions for filing a claim please type or print using black ink for each eligible family member, dependent or spouse separate all itemized...
FILL NOW