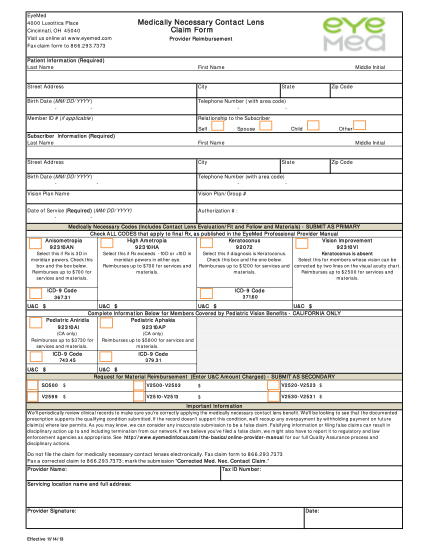
Claim Form - Medical for California participants - dgaplans
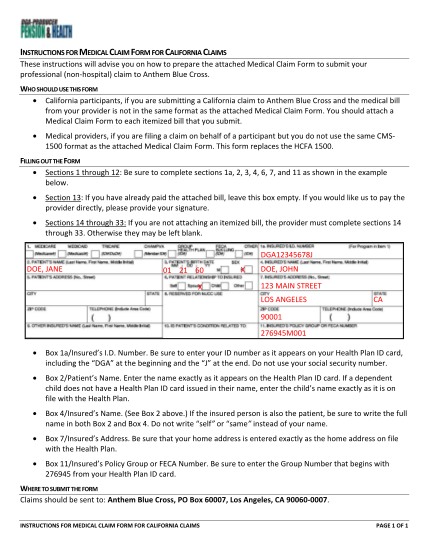
Instructions for medical claim form for california claims these instructions will advise you on how to prepare the attached medical claim form to submit your professional (nonhospital) claim to anthem blue cross. who should use this form...
FILL NOW