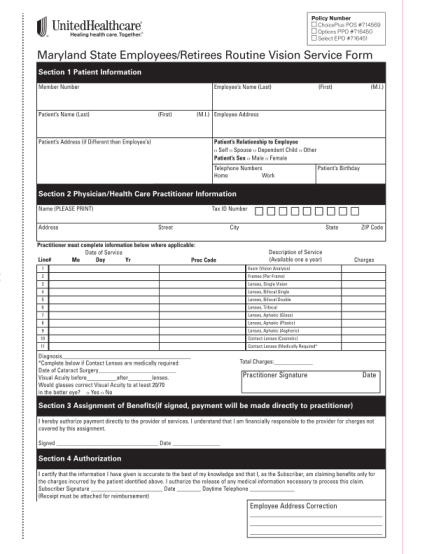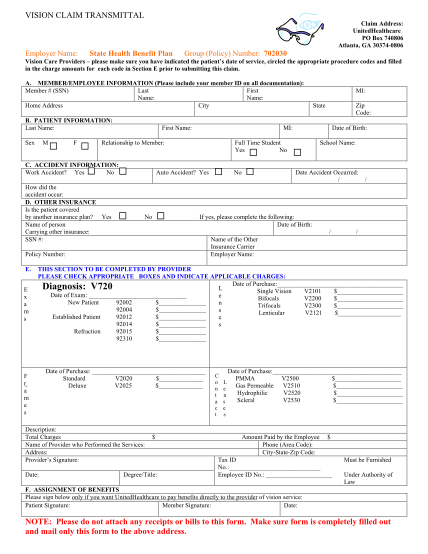
Fillable health insurance claim form 1500 united healthcare - adp fsa claim form
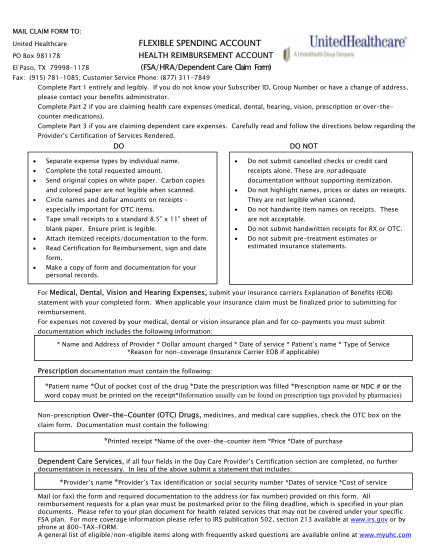
Submitting your health care fsa claim how to file a health care claim to complete a health care reimbursement request (a claim), you must submit a health care fsa claim form along with the receipts that clearly show an eligible expense was...
FILL NOW