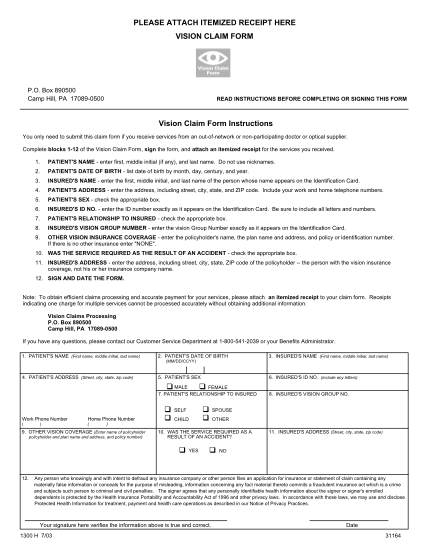
carefirst vision claim form
Vision/eye care claim form patient and subscriber information 1. patient's name (first, middle initial, last name) 2. patient's date of birth 3. subscriber's name (first, middle initial, last name) 4. patient's other insurance information is...
FILL NOW