foundation medicine medical release form
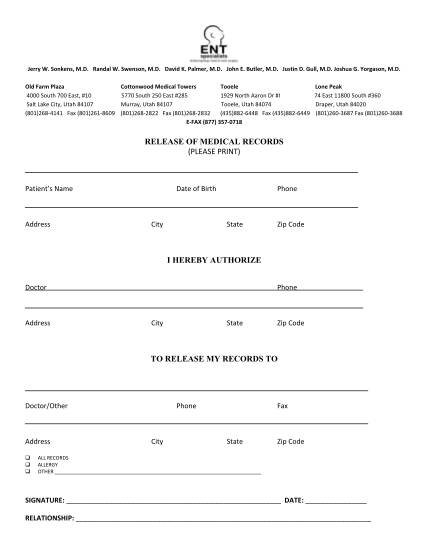
Innovative healthcare solutions. world trade center national responder health program medical records release form patient name (please print) wtc number date of birth (mm/dd/y) i authorize: name of sending person/organization: address: city,...
FILL NOW