authorization release information
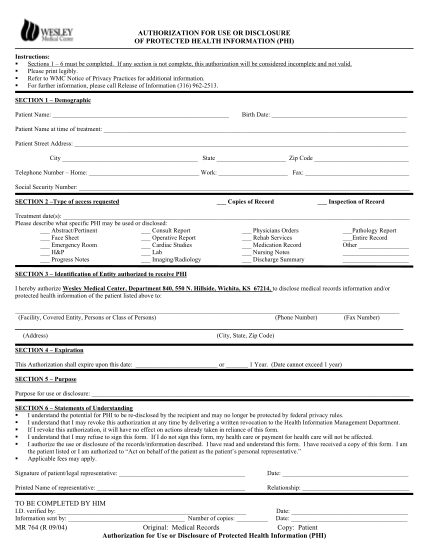
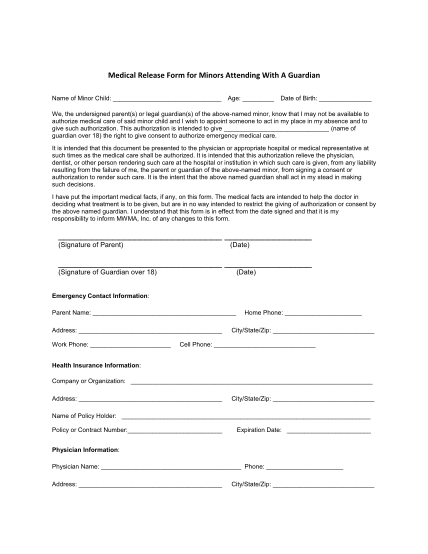
Date: id verification (type): patient name: birthdate: id verified by: authorization for release of health information i authorize the purpose of this release is (name of person or facility which has information - example: ucsf/mt. zion) for...
FILL NOW