Client Medical History Form - IMagic Beauty
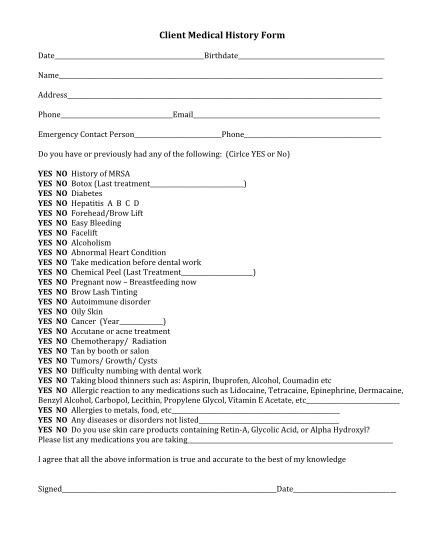
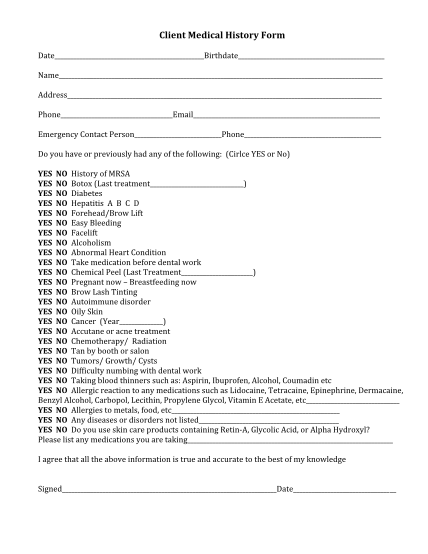
Client 'medical 'history 'form '! date birthdate ! ! name ! ! address ! ! phone email ! ! emergency!contact!person phone ! ! do!you!have!or!previously!had!any!of!the!following:!!(cirlce!yes!or!no)! ! yes ' 'no!!history!of!mrsa! yes '...
FILL NOW