Ord rEC alth hE Child - bfostercaretxcomb
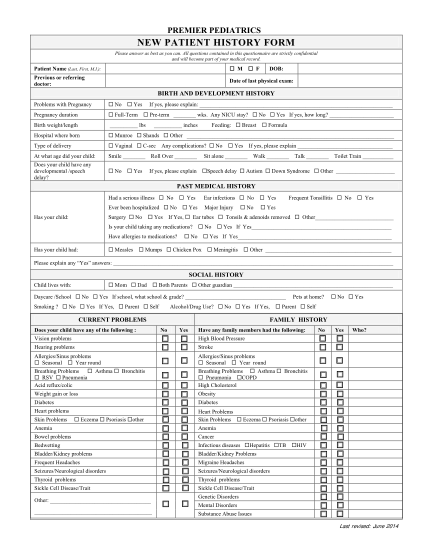
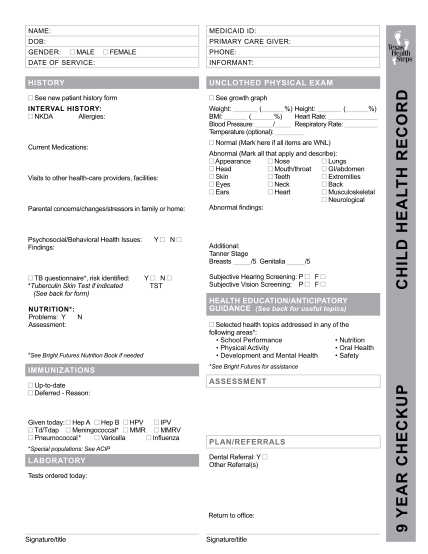
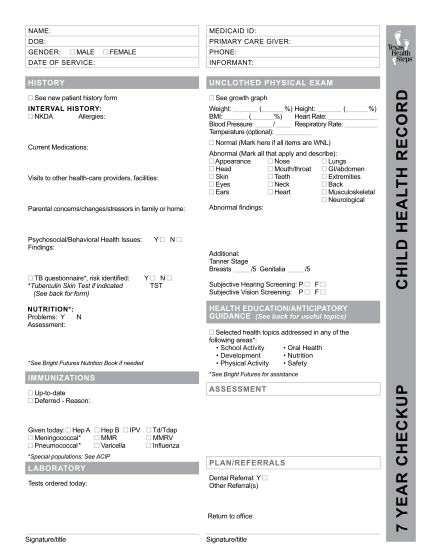
Name: medicaid id: dob: primary care giver: gender: male female phone: informant: history unclothed physical exam see new patient history form see growth graph interval history: nkda allergies: ( weight: ( %) height: bmi: ( %) heart rate: blood...
FILL NOW