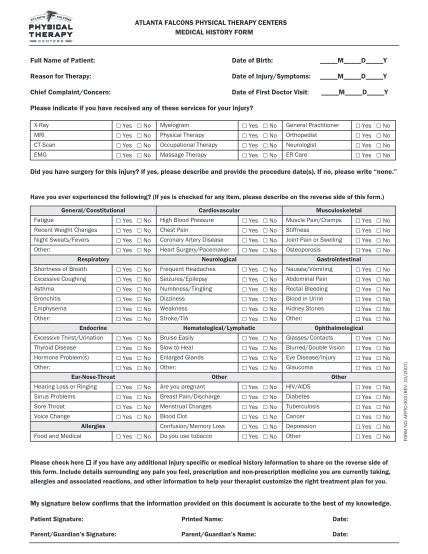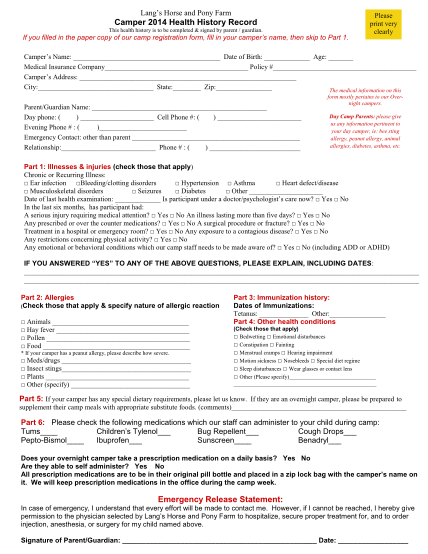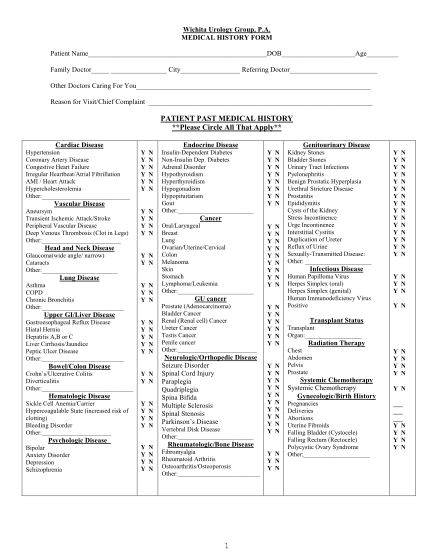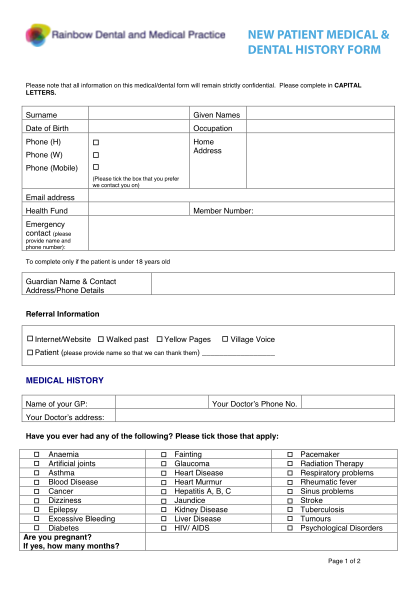
Basic medical history form - medical history questionnaire
6560 fannin,#450 houston,tx 77030 713-441-8843; fax 713-793-1636 date medical history questionnaire general ophthalmology methodist eye associates requests this information for the purpose of providing patient care. no persons outside tmh are...
FILL NOW