New Patient Health Records bFormb - Suncoast Cancer Institute
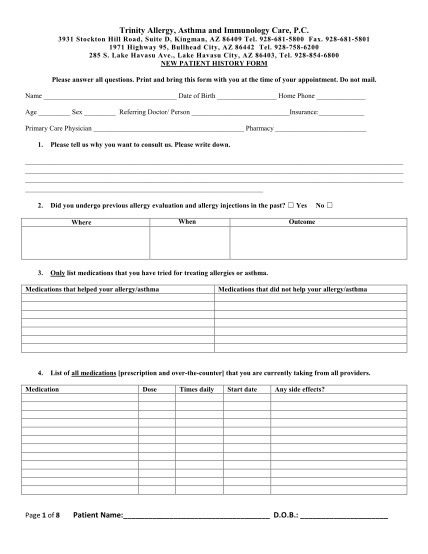
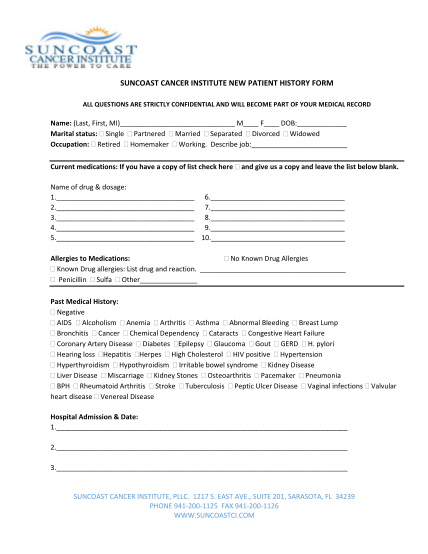
Suncoast cancer institute new patient history form all questions are strictly confidential and will become part of your medical record name: (last, first, mi) m f dob: marital status: single partnered married separated divorced widowed occupation:...
FILL NOW