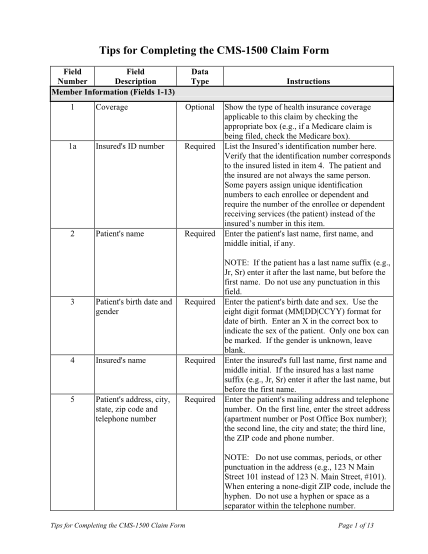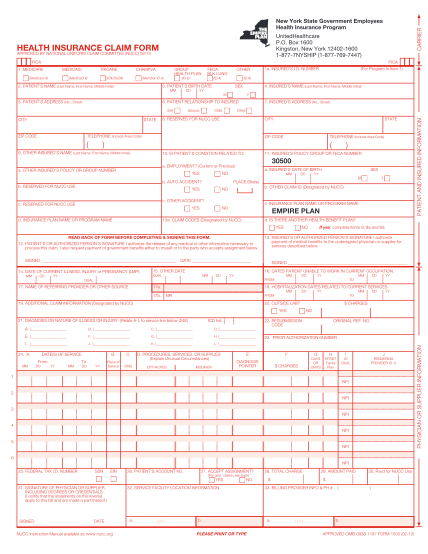
cms 1500 claim form
Health insurance claim form. note: claims must be submittedwithin 3 months of being incurred to be eligible forreimbursement. 1. insured's name (last name, first name, middle initial). 8.patient's name (last name, first name, middle initial). 9....
FILL NOW