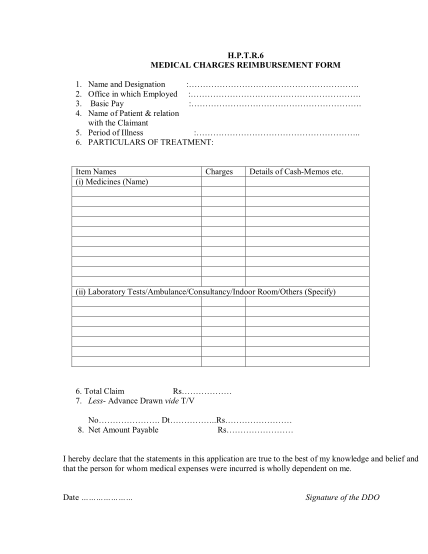
CHISF01 - Claim for reimbursement of medical expenses CERN CHIS UNIQA Claim Reimbursement
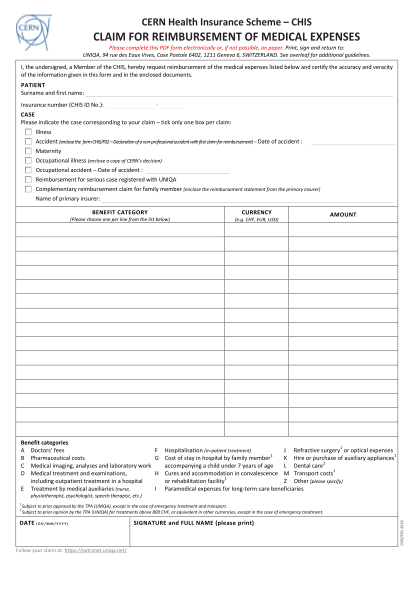
Cern health insurance scheme chis claim for reimbursement of medical expenses please complete this pdf form electronically or, if not possible, on paper. print, sign and return to: uniqa, 94 rue des eaux vives, case postale 6402, 1211 geneva 6,...
FILL NOW