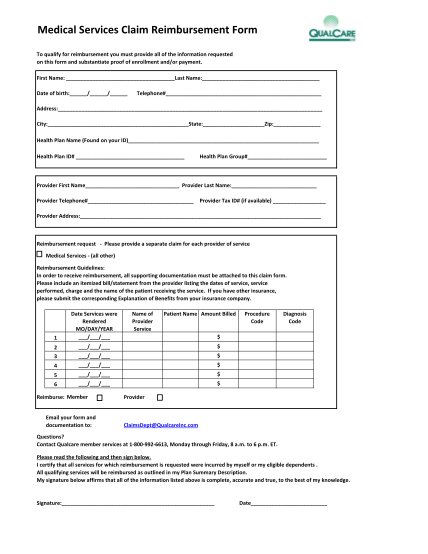
qualcare medical claim form
Medical services claim reimbursement form to qualify for reimbursement you must provide all of the information requested on this form and substantiate proof of enrollment and/or payment. first name: last name: date of birth: / / telephone#...
FILL NOW