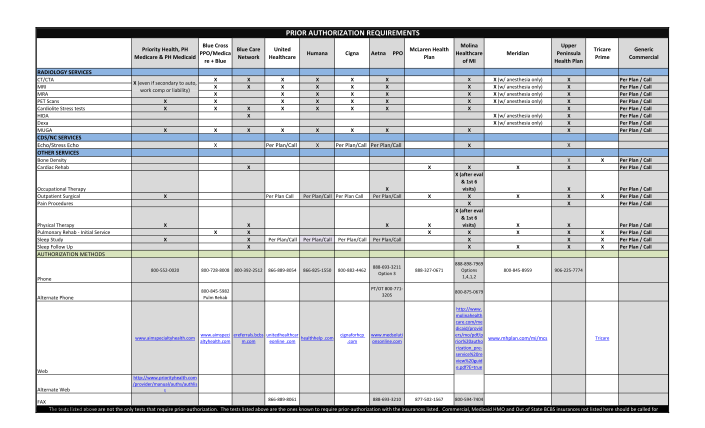
mclaren prior authorization form
Prior authorization requirements priority health, ph medicare & ph medicaid blue cross ppo blue care network united healthcare humana cigna x x x x x x x x x x x x x x x x x x x x x x x x x x x radiology services ct/cta mri mra pet scans stress...
FILL NOW