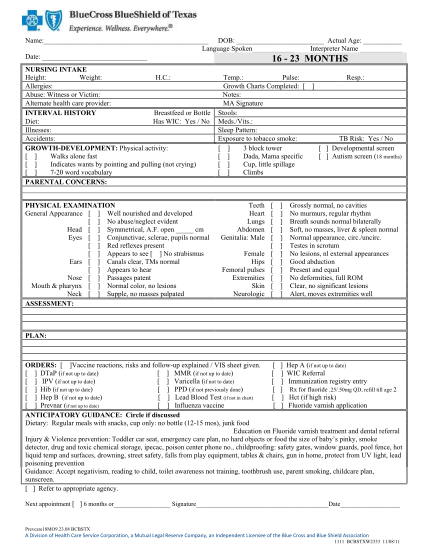
Language Spoken
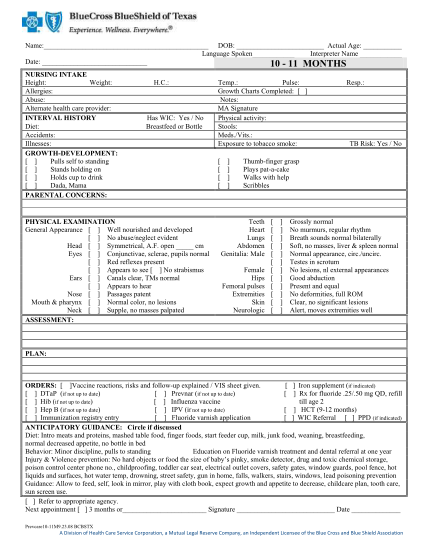
Name: dob: actual age: language spoken interpreter name date: 16 23 months nursing intake height: weight: h.c.: allergies: abuse: witness or victim: alternate health care provider: interval history breastfeed or bottle diet: has wic: yes / no...
FILL NOW