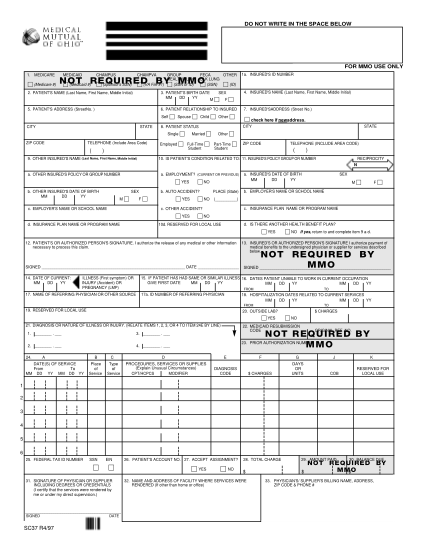
40b medicare form
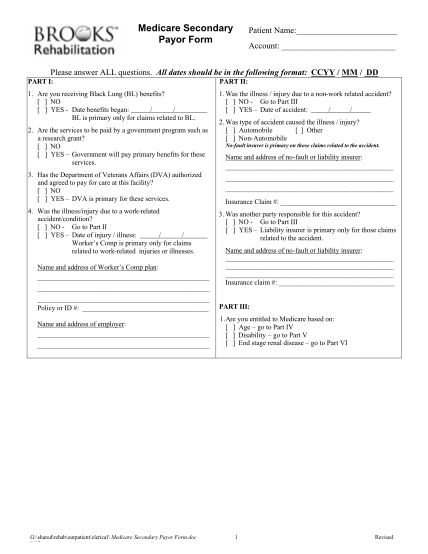
Medicare secondary payor form patient name: account: please answer all questions. all dates should be in the following format: ccyy / mm / dd part i: 1. are you receiving black lung (bl) benefits? no yes - date benefits began: / / bl is primary...
FILL NOW