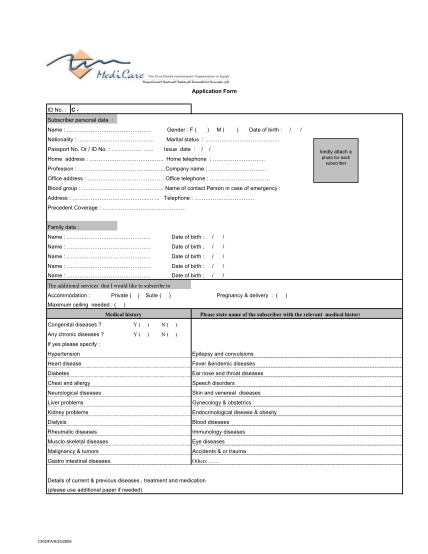
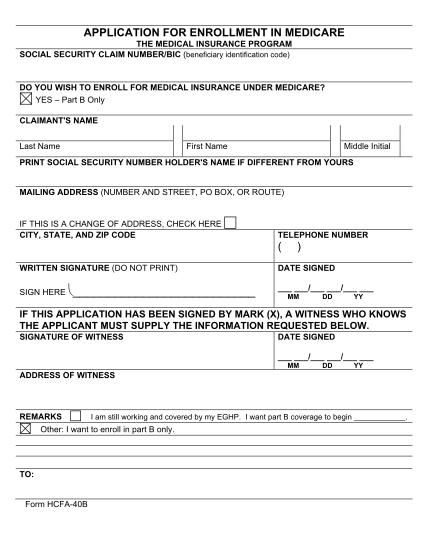
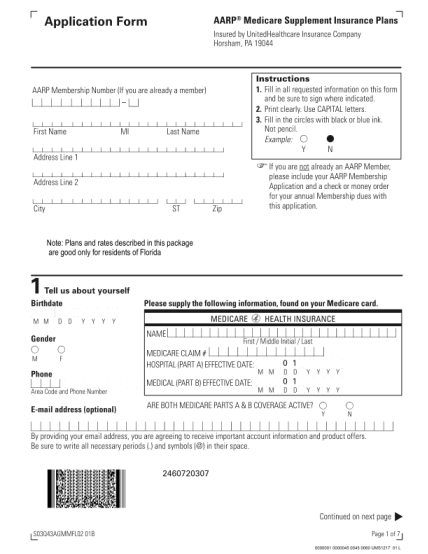
3101 - Medicare enrolment application form. Application to copy or transfer from one Medicare card to another - bw
Student activities office 2nd floor strosacker college union 275 eastland rd berea, oh 44017 (440) 826-2356 office stuact bw.edu five stages of group/ team development stage one: to be of not to be: forming, orientation or familiarity stage: this...
FILL NOW