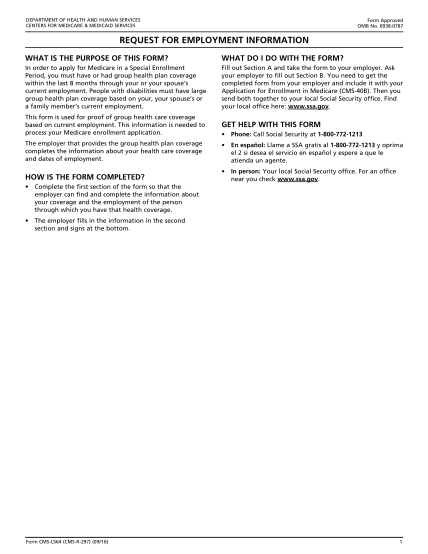
APPLICATION FOR ENROLLMENT IN MEDICARE PART B ... - cms
part a, do not complete this form. contact social security if you want to apply for medicare for form cms-l564 request for employment information completed by your near you check .ssa.gov. reminders cms-40b ( 04/17). 1
FILL NOW