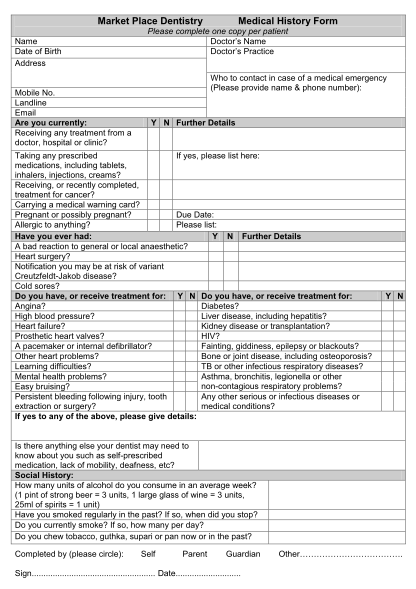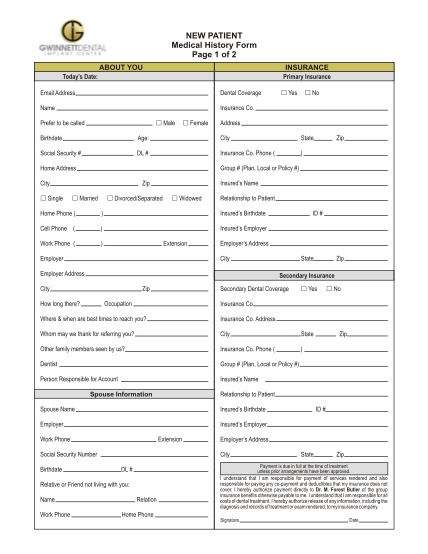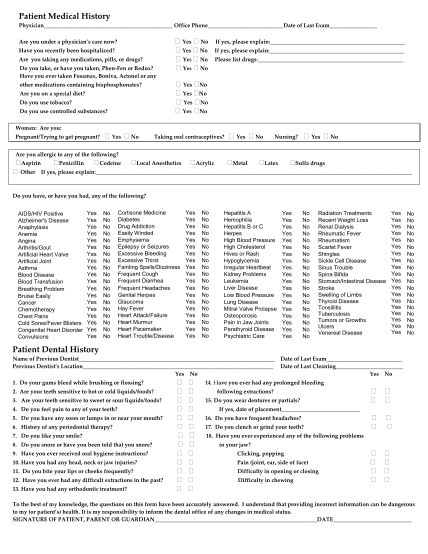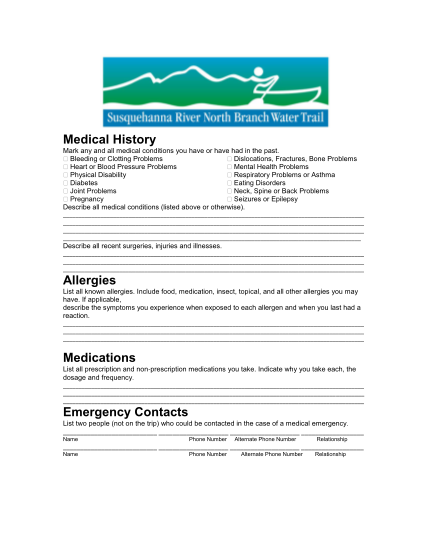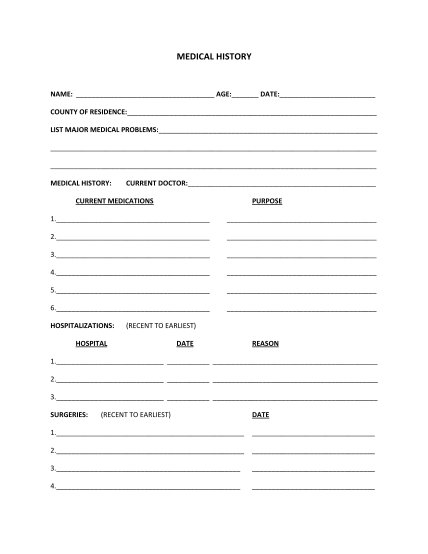
General Medical History Form - Wayne Bonlie, M.D.
Please use as much space as needed to answer questions. if you are filling in this form by hand and not on the computer, please use the back of the page or use additional pages if needed. you may fax or email this information to me prior to your...
FILL NOW