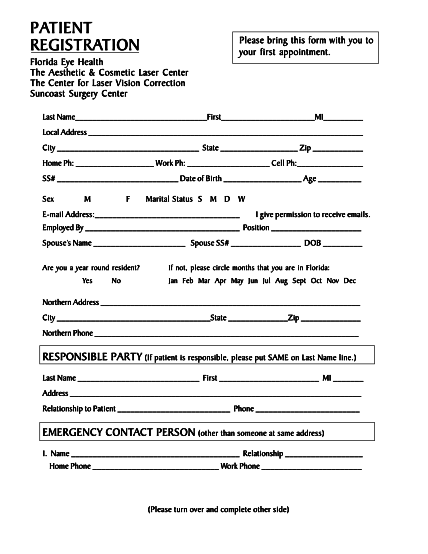
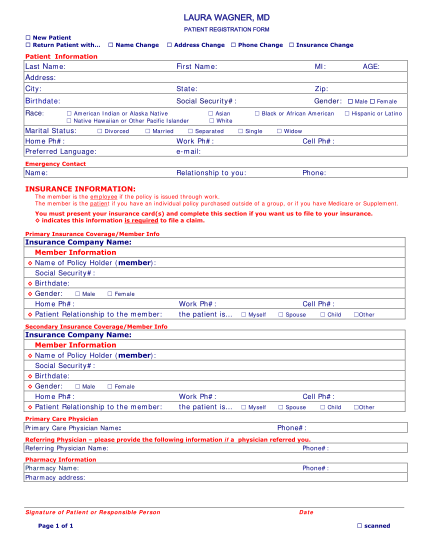
new patient forms
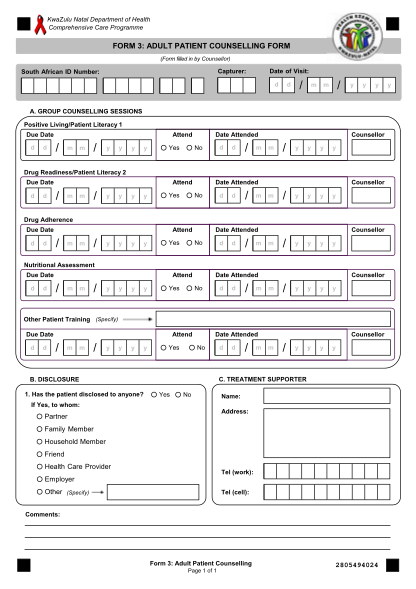
Patient registration form **today s date: clinic name: patient information: (please use full legal name, no nicknames) *last name: *first name: middle initial: *address: city: state: zip: home phone #: ( ) - *social security #: *date of birth:...
FILL NOW