PATIENT REGISTRATION-HIPAA FORM 2 revised 07-2008doc
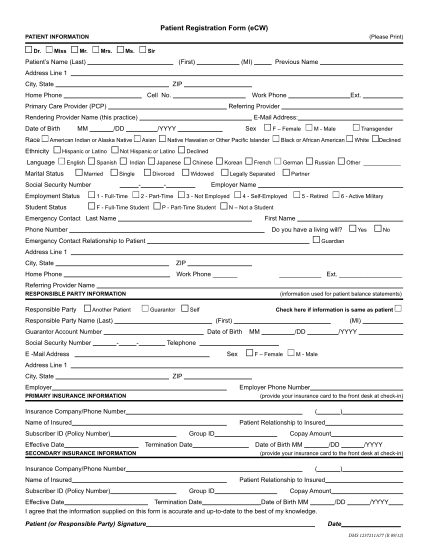
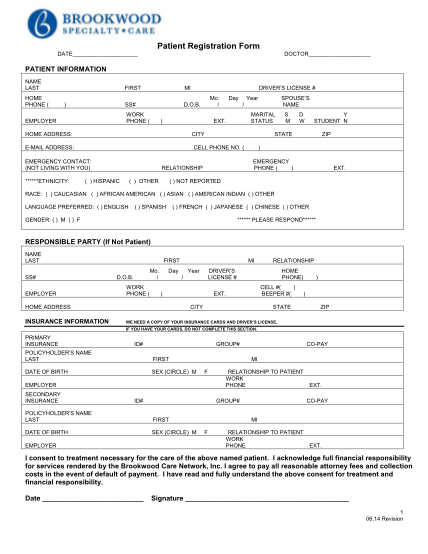
Pediatric healthcare, llc 4700 woodmere boulevard, montgomery, al 36106 phone: 3342739700 fax: 3342739788 martin c. glover, m.d. david l. morrison, m.d den a. trumbull, m.d. jeffrey a. simon, m.d. patient registration form (please print all...
FILL NOW