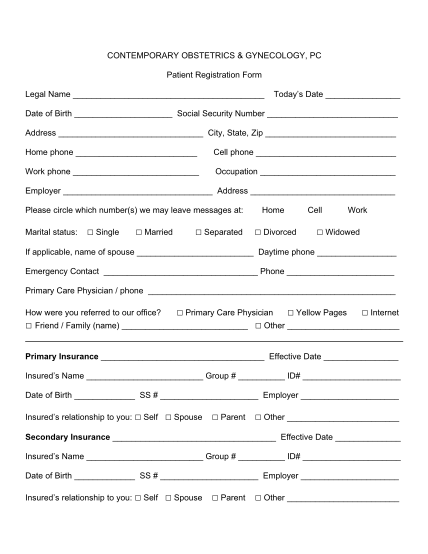
demographic sheet template
Vascular and endovascular institute of orange county gary nishanian, md, rvt, facs 26800 crown valley pkwy, suite 420 mission viejo, ca 92691 patient information: date: name: address: age: sex: a medical corporation phone: (949) 429-8840 fax:...
FILL NOW