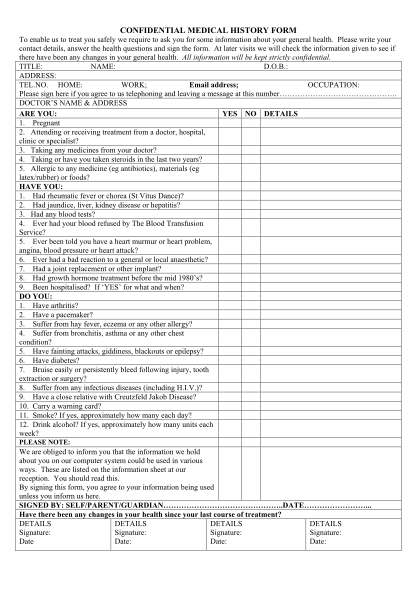
New Patient Information and Medical History Forms - Dowell Dental ...
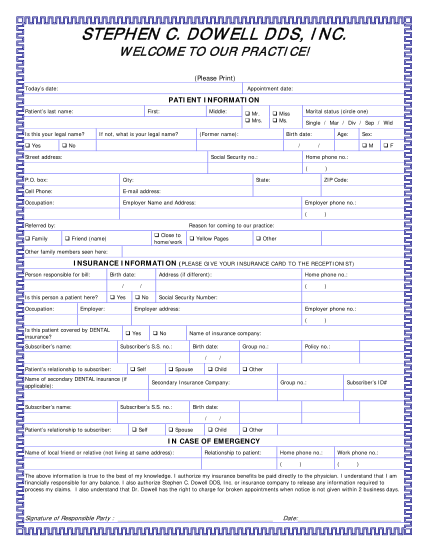
Stephen c. dow ell dds, i nc. w elcom e to our p r acti ce! (please print) today s date: appointment date: patient information patient s last name: first: is this your legal name? ? yes middle: if not, what is your legal name? ? mr. ? mrs. marital...
FILL NOW