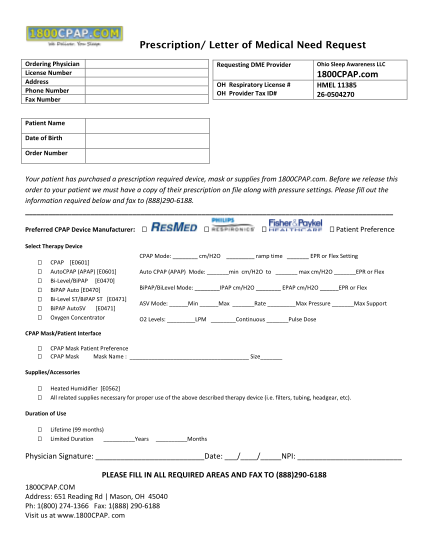
1800cpap consultation form
Prescription/ letter of medical need request ordering physician license number address phone number fax number requesting dme provider ohio sleep awareness llc 1800cpap.com oh respiratory license # oh provider tax id# hmel 11385 260504270 patient...
FILL NOW